

Abstract
Background Urolithiasis is a common cause of urinary tract obstruction and urinary tract infection (UTI). This study aimed to identify whether urolithiasis with or without hydronephrosis has an impact on acute kidney injury (AKI) in patients with UTI.
Methods and findings This retrospective study enrolled hospitalized UTI patients who underwent imaging in an acute care setting from January 2006 to April 2019. Of the 1113 participants enrolled, 191 (17.2%) had urolithiasis and 76 (6.8%) had ureteral stone complicated with hydronephrosis. Multivariate logistic regression analysis showed that in UTI patients with urolithiasis, the presence of ureteral stone with concomitant hydronephrosis was an independent risk factor for AKI (odds ratio [OR] 2.345, 95% confidence interval [CI] 1.128–4.876, P = 0.023). In addition, urolithiasis was associated with an increased risk for AKI (OR 2.484, 95% CI 1.398–4.415, P = 0.002) in UTI patients without hydronephrosis.
Conclusion The presence of ureteral stone with hydronephrosis increases the risk for AKI of UTI patients with urolithiasis, and urolithiasis remains a risk factor of AKI in UTI patients without hydronephrosis.
Introduction
Urolithiasis is a widespread problem with a male preponderance, showing a lifetime prevalence of 10% in men and 5% in women [1, 2]. The worldwide prevalence of urolithiasis is also steadily increasing [1-3], partially owing to its strong association with metabolic syndrome conditions such as obesity, hypertension, and diabetes [4].
Urolithiasis can cause secondary complications, such as obstruction or urinary tract infection (UTI) [5]. Acute UTI may cause sudden deterioration of renal function, especially in the presence of urinary tract obstruction [6]. Our previous study showed that urolithiasis is a risk factor for acute kidney injury (AKI) among patients with UTI [7], and AKI has been associated with short- and long-term mortality [8]. Since AKI leads to poor outcomes, recognizing the risk factors for its development in patients with urolithiasis and UTI is crucial. However, no study has focused on whether urolithiasis without hydronephrosis is a risk factor for the development of AKI in patients with UTI, or whether hydronephrosis caused by ureteral stone is a risk factor for the development of AKI in UTI patients with urolithiasis. Hence, we conducted this study to investigate these important issues.
Methods
Patient selection
This retrospective observational study covered the period from January 2006 to April 2019 and was conducted at Chia-Yi Christian Hospital, a tertiary referral center in the southwestern part of Taiwan. This study was performed after obtaining ethical approval from the Institutional Review Board of Chiayi Christian Hospital (approval no. CYCH-IRB-2019061).
A total of 1113 consecutive hospitalized patients with UTI without any other concurrent infectious disease were enrolled. All enrolled patients fulfilled the following criteria: (a) with UTI symptoms and > 105 colony-forming units/mL of bacterial isolates from a urine specimen; (b) had available antimicrobial susceptibility test results; and (c) underwent complete imaging examination, including ultrasonography, intravenous urography, or computed tomography, and had complete data of the required laboratory tests. Patients aged < 18 years, with concurrent infection other than UTI, without imaging studies, with incomplete data, or undergoing regular dialysis therapy were excluded from this study. The included patients were divided into three groups: UTI patients with no hydronephrosis or urolithiasis, UTI patients with ureteral stone and concomitant hydronephrosis, or UTI patients with urolithiasis but no hydronephrosis (Fig 1).

Inpatients were assessed using standard laboratory and diagnostic procedures. For further analysis, we collected clinical data in a standard form, including demographic characteristics (age and sex), comorbidities (coronary artery disease, congestive heart failure [CHF], stroke, diabetes mellitus [DM], or hypertension), presence of an indwelling Foley catheter, vital signs (blood pressure and ear temperature), laboratory results (white blood cell [WBC] count, platelet count, serum creatinine level, and estimated glomerular filtration rate [eGFR] at baseline and after hospitalization), prior history of UTI, existence of a urinary tract abnormality (urolithiasis or hydronephrosis), length of hospital stay, causative microorganisms (Escherichia coli [E. coli], Proteus species, Klebsiella species, Enterococcus species, and Pseudomonas species), and antimicrobial resistance pattern.
Definition and examples of clinical covariates
The eGFR was determined using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation and expressed in mL/min/1.73 m2 [9, 10]. AKI was defined as an increase in serum creatinine to ≥ 2.0 times the baseline value according to the Kidney Disease: Improving Global Outcomes Clinical Practice Guideline criteria for serum creatinine value for AKI stages 2 and 3 [11]. Hydronephrosis was defined as dilatation of the renal pelvis and calyces in imaging studies. Uroseptic shock was defined as sepsis-induced hypotension (systolic blood pressure [SBP] < 90 mmHg or mean arterial pressure < 70 mmHg or a decrease in SBP by > 40 mmHg lasting for at least 1 hour, despite adequate fluid resuscitation and in the absence of other causes of hypotension) [12]. An afebrile status was defined as a single temperature not increasing to > 38.3°C (101°F) [13]. Multiple drug resistance (MDR) was defined as non-susceptibility to at least three antimicrobial categories [14].
Statistical analysis
All analyses were performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). Continuous variables are expressed as mean ± standard deviation, and categorical variables are expressed as number (percentage). Univariate analyses were performed using Student’s t-test for continuous variables, and the chi-square test and Fisher’s exact test for categorical variables. Multivariate logistic regression analyses were applied to identify risk factors associated with AKI during hospitalization. Only variables significant at the 0.15 level in univariate analysis were selected for the subsequent multivariate analysis. The goodness-of-fit of the logistic regression model was assessed using the Cox & Snell test, and the explanatory power was reported with Nagelkerke’s pseudo-R-square. P < 0.05 was considered statistically significant.
Results
Characteristics of the study population
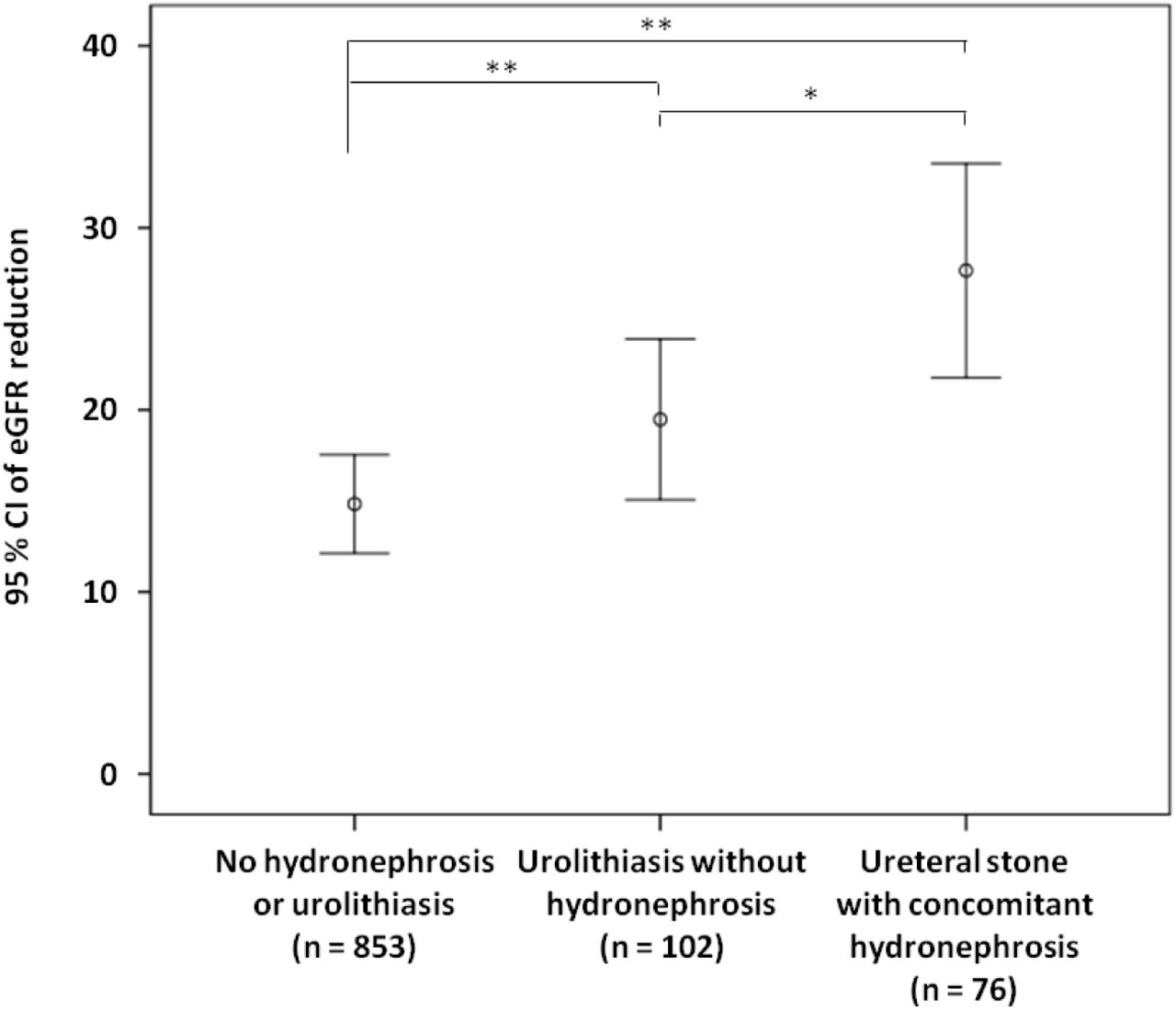
The demographic and clinical characteristics of the 1113 hospitalized UTI patients included in this study are shown in Table 1. The mean age on admission was 66 ± 17 years. Most of the patients (816 [73.3%]) were women, and 375 (33.7%) had a history of prior UTI. Of the patients, 220 (19.8%) had uroseptic shock and 165 (14.8%) had AKI during hospitalization. The overall mortality rate was 0.6% (7/1113). Among UTI patients, 191 (17.2%) had urolithiasis and 76 (6.8%) had ureteral stone with hydronephrosis. Fig 2 shows a reduction in eGFR in different groups of hospitalized patients with UTI. The reduction in eGFR in UTI patients without urolithiasis or hydronephrosis, in those with urolithiasis but without hydronephrosis, and in those with ureteral stone and concomitant hydronephrosis was 13.45 (95% confidence interval [CI] 12.44–14.45), 20.54 (95% CI 16.34–24.73), and 27.65 (95% CI 21.77–33.53) mL/min/1.73 m2, respectively. Thirteen urolithiasis patients who had hydronephrosis but with no ureteral stone identified in imaging studies and 69 patients who did not have urolithiasis but had hydronephrosis were excluded from further analysis (Fig 1).
Characteristics of hospitalized patients with urinary tract infection with respect to urolithiasis
{kind=link}
{kind=link}
eGFR: estimated glomerular filtration rate. UTI: urinary tract infection. eGFR reduction: baseline minus worst value of eGFR. *P <0.05, **P <0.01.
Risk factors of hospitalized UTI patients with urolithiasis with respect to ureteral stone and concomitant hydronephrosis
The demographic and clinical characteristics of UTI patients with urolithiasis are shown in Table 2. Patients with ureteral stone and concomitant hydronephrosis had higher serum creatinine level on admission (2.35 ± 2.28 versus 1.58 ± 1.41 mg/mL, P = 0.02), longer hospital stay (12 ± 6 versus 9 ± 4 days, P < 0.001), higher prevalence of bacteremia (69.7% versus 49.0%, P = 0.006) and AKI (40.8% versus 22.5%, P = 0.009), and lower prevalence of afebrile status (19.7% versus 40.2%, P = 0.004) than those without ureteral stone and concomitant hydronephrosis. Univariate logistic regression analysis showed that older age (odds ratio [OR] 1.032, 95% CI 1.006–1.057, P = 0.014), uroseptic shock (OR 6.249, 95% CI 3.074–12.702, P < 0.001), and ureteral stone with concomitant hydronephrosis (OR 2.366, 95% CI 1.233–4.541, P = 0.01) were associated with an increased risk for AKI, whereas a higher platelet count (OR 0.995, 95% CI 0.991–1.000, P = 0.042) was associated with a decreased risk for AKI in UTI patients with urolithiasis. Multivariate logistic regression analysis revealed that older age (OR 1.032, 95% CI 1.002–1.063, P = 0.038), uroseptic shock (OR 4.769, 95% CI 2.184–10.412, P < 0.001), and ureteral stone with concomitant hydronephrosis (OR 2.345, 95% CI 1.128–4.876, P =0.023) were independently associated with an increased risk for AKI in UTI patients with urolithiasis (Table 3).
Characteristics of hospitalized urinary tract infection patients with urolithiasis with respect to ureteral stone with hydronephrosis
Univariate and multivariate logistic regression analyses of factors related to acute kidney injury in hospitalized urinary tract infection patients with urolithiasis
Risk factors of hospitalized UTI patients without hydronephrosis with respect to urolithiasis
The demographic and clinical characteristics of UTI patients without hydronephrosis are shown in Table 4. Patients with urolithiasis had a higher prevalence of male gender (38.2% versus 25.3%, P = 0.005), prior history of UTI (45.1% versus 31.4%, P = 0.016), AKI (22.5% versus 9.6%, P < 0.001), and Proteus species (7.8% versus 1.6%, P = 0.001), but a lower prevalence of E. coli (72.5% versus 80.9%, P = 0.047), than those without urolithiasis. Univariate logistic regression analysis showed that older age (OR 1.029, 95% CI 1.015–1.043, P < 0.001), DM (OR 1.549, 95% CI 1.031–2.326, P = 0.035), hypertension (OR 2.596, 95% CI 1.665–4.048, P < 0.001), CHF (OR 2.691, 95% CI 1.282–5.646, P = 0.009), afebrile status (OR 1.556, 95% CI 1.034–2.340, P = 0.034), bacteremia (OR 1.696, 95% CI 1.128–2.550, P = 0.011), uroseptic shock (OR 4.318, 95% CI 2.814–6.627, P < 0.001), urolithiasis (OR 2.737, 95% CI 1.632–4.591, P < 0.001), and higher WBC count (OR 1.059, 95% CI 1.027–1.092, P < 0.001) were associated with an increased risk for AKI, whereas a higher baseline eGFR (OR 0.982, 95% CI 0.976–0.989, P < 0.001) was associated with a decreased risk for AKI in UTI patients without hydronephrosis. Multivariate logistic regression analysis revealed that hypertension (OR 2.064, 95% CI 1.226–3.475, P = 0.006), uroseptic shock (OR 4.505, 95% CI 2.798–7.253, P < 0.001), urolithiasis (OR 2.484, 95% CI 1.398–4.415, P = 0.002), and higher WBC count (OR 1.061, 95% CI 1.027–1.096, P < 0.001) were independently associated with an increased risk for AKI in UTI patients without hydronephrosis. Conversely, a higher baseline eGFR (OR 0.985, 95% CI 0.977–0.994, P = 0.001) was independently associated with a decreased risk for AKI in UTI patients without hydronephrosis (Table 5).
Characteristics of hospitalized urinary tract infection patients without hydronephrosis with respect to urolithiasis
Univariate and multivariate logistic regression analyses of factors related to acute kidney injury in urinary tract infection patients without hydronephrosis
Discussion
UTI is a common complication in patients with urolithiasis. Urolithiasis is a common cause of urinary tract obstruction predisposing to UTI [15]. A previous study showed that urinary obstruction is a predictor of the development of septic shock in UTI patients [16]. In this study, we identified that the presence of ureteral stone with hydronephrosis is a risk factor for AKI in UTI patients with urolithiasis. In addition, urolithiasis is a risk factor for AKI in UTI patients without hydronephrosis. To our knowledge, this is the first study to demonstrate that urolithiasis without hydronephrosis is associated with an increased risk for AKI in patients with UTI.
Urolithiasis is a major cause of obstructive pyelonephritis, accounting for 65% of obstructive pyelonephritis events [17]. Urinary stasis provides the time and opportunity for bacteria to adhere to the urothelium, multiply, and infect the host [18]. In addition, stones moving down the ureter result in inflamed narrowing of the ureter or injuries, which could easily cause infection [19]. Obstructive uropathy is not a rare cause of UTI. A previous study showed that the rate of obstructive uropathy in patients clinically diagnosed with a simple pyelonephritis was approximately 6% [20]. Obstructive UTI is associated with a high recurrence rate. In a long-term follow-up study in patients with obstructive pyelonephritis, the incidence of recurrent obstructive pyelonephritis and recurrent UTI was 11% and 33%, respectively [17]. The existence of ureteral stone is the most common cause of urosepsis in patients with urinary tract obstruction [16]. UTI in the presence of urinary tract obstruction is a serious clinical situation. In the case of acute obstructive uropathy, the increased intrarenal pelvic pressure decreases the drug delivery to the kidney [21]. Both urolithiasis and obstructive uropathy have an impact on the severity of urosepsis [22], the presence of urinary tract obstruction in patients with acute pyelonephritis is associated with an increased risk for urosepsis and uroseptic shock [23, 24]. In the current study, the presence of ureteral stone with hydronephrosis was an independent risk factor for AKI development in UTI patients with urolithiasis.
Obstructive nephropathy is the major cause of non-infectious urolithiasis associated AKI [25]. Renal vasoconstriction and inflammation can occur in response to increased intratubular pressure, and cause ischemia injury. If ischemia persists, glomerulosclerosis, tubular atrophy, and interstitial fibrosis occur [26]. In a rat model, complete unilateral obstruction for 24 hours resulted in irreversible loss of function in 15% of the nephrons of the affected kidney [27]. Obstructive AKI caused by urolithiasis is not common, accounting for only approximately 1–2% of all AKI events [25]. A previous study reported that the prevalence of AKI among patients with non-infectious ureteral stone was 0.72% [28]. Infection is one of the leading causes of AKI in patients with ureteral stone [29], and infection with concomitant obstructive uropathy causes loss of function far more rapidly than a simple obstructive uropathy [30]. Yamamoto et al. found that approximately 80% of patients with acute obstructive pyelonephritis induced by upper ureteral stone had elevated serum creatinine levels above the normal range [31]. AKI is associated with an increased risk for mortality in patients with upper ureteral stone with concomitant urosepsis [32]. Untreated infection with concomitant urinary tract obstruction can lead to life-threatening sepsis. After the administration of appropriate antibiotics, interventions, such as drainage for source control, should be performed within 12 hours after the diagnosis of sepsis, according to the recommendation from the Surviving Sepsis Campaign 2016 [33]. The management of infected hydronephrosis secondary to urolithiasis is prompt decompression of the renal collecting system [34]. Optional methods of decompression include percutaneous nephrostomy and retrograde ureteral stenting [22]. Decompression of the renal collecting system increases the renal plasma flow and delivery of antibiotics to both the renal parenchyma and urine [35]. Moreover, the release of inner pressure from the upper urinary tracts reduces the invasion of bacteria into the bloodstream or renal parenchyma [36]. Both the increase of antibiotic penetration into the affected renal unit and the decrease of bacterial invasion can facilitate infection control. Further, the severity of tubular atrophy and interstitial fibrosis increases if the duration of obstruction is extended [37], and a delayed relief of ureteral obstruction decreases long-term renal function [38]. If obstruction is relieved early and infection is controlled, the renal parenchyma has a great potential for recovery [29]. Delay or omission of renal decompression will increase the rate of sepsis and mortality [17]. Because UTI patients with concomitant ureteral stone resulting in urinary tract obstruction are predisposed to develop severe complications, such as septic shock or AKI, timely decompression of the renal collecting system through percutaneous nephrostomy or retrograde ureteral stenting after starting empiric antibiotic therapy is recommended for those with a critical status [39].
Urolithiasis is a source of infection [40], and UTIs are frequently associated with almost all chemical types of kidney stones [41]. Urolithiasis is the one of most common urological disorders associated with complicated pyelonephritis [42] and is also a risk factor for treatment failure in patients with acute pyelonephritis [43]. Because the amount of bacteria on the stone surface can increase despite antibiotic therapy, eradication of the associated UTI is only possible after the stone has been completely removed [44]. According to the Nationwide Inpatient Sample survey between 1999 and 2009, the incidence of urolithiasis-associated sepsis and severe sepsis is increasing [45]. Urolithiasis is also a risk factor of septic shock in patients with UTI [7], and sepsis is one of the most common etiologies of AKI [46]. In the current study, urolithiasis without hydronephrosis was associated with an increased risk for AKI in patients with UTI. Early imaging examination to identify urolithiasis and complete removal of urolithiasis after ameliorating the symptoms of sepsis are crucial for patients with UTI.
Our study had several limitations. First, this was a single-center study with a retrospective design. A multicenter prospective study with a larger sample size will be needed to confirm our results. Second, we did not routinely examine the stone characteristics in this study. Further studies evaluating the chemical types of stones will be needed to confirm their impact on AKI in patients with UTI.
Conclusions
We demonstrated that patients with ureteral stone complicated with hydronephrosis have a higher risk of developing AKI among UTI patients with urolithiasis, and urolithiasis remains a risk factor for AKI among UTI patients without hydronephrosis. Therefore, timely decompression of the renal collecting system for infectious hydronephrosis secondary to urolithiasis and complete stone removal after controlling infection are crucial for UTI patients with urolithiasis.
Author Contributions
Conceptualization: Chih-Yen Hsiao.
Data curation: Chih-Yen Hsiao.
Formal analysis: Yi-Chien Lee and Tsung-Hsien Chen.
Methodology: Chih-Yen Hsiao.
Supervision: Ming-Cheng Wang.
Writing – original draft: Chih-Yen Hsiao, and Tsung-Hsien Chen.
Writing – review & editing: Ming-Cheng Wang.
Competing interests
The authors have declared that no competing interests exist.
Acknowledgments
The authors would like to acknowledge the support of Cheng-Lun Chiang.
References




