

Abstract
Remdesivir, an investigational broad-spectrum antiviral agent, has shown in vitro activity against SARS-CoV-2. To maximize direct delivery to the target site, the lungs, we aim to develop remdesivir as a dry powder for inhalation using thin film freezing (TFF). TFF produces a brittle matrix of nanostructured aggregates that can be sheared into respirable low-density microparticles upon aerosolization from a passive dry powder inhaler. In vitro aerodynamic testing demonstrated that drug loading and excipient type affected the aerosol performance of remdesivir. Remdesivir combined with optimal excipients (e.g. Captisol®, mannitol, lactose, leucine) exhibited suitable aerosol performance (up to 92.4% FPF and 0.86 µm MMAD). Remdesivir was amorphous after the TFF process, which we hypothesize will provide a benefit for drug dissolution once administered to the lungs. Neither the organic/water processing cosolvent or the rapid freezing rate used during the TFF process affected the chemical stability of remdesivir during processing. In conclusion, TFF is a suitable technology for producing remdesivir dry powder formulations suitable for pulmonary administration.
1. Introduction
The coronavirus disease 2019 (COVID-19) has become an ongoing worldwide pandemic. As of July 2020, laboratory-confirmed cases have been reported in 213 countries and territories with more than 15 million reported cases and more than 600,000 reported deaths (1). Although this disease is asymptomatic to mild in most people, in some cases, it can develop into pneumonia, acute respiratory distress syndrome (ARDS) and multi-organ dysfunction (2). While effective treatments for COVID-19 are urgently needed, there are currently no drugs approved to treat COVID-19. Only one drug, remdesivir administered by intravenous (IV) injection, has been authorized for emergency use in adult and pediatric patients hospitalized with severe disease. Therefore, additional therapeutics and routes of administration are needed to treat this virus.
Remdesivir (GS-5734), an investigational broad-spectrum antiviral agent, has been developed by Gilead Sciences Inc. (3). Remdesivir is a monophosphoramide prodrug that is intracellularly metabolized into an adenosine triphosphate analog (GS-441524) (4). Both GS-411524 and remdesivir (GS-5734) are metabolized into the active nucleoside triphosphate (GS-443902) by the host (5). The adenosine nucleoside analog can inhibit viral RNA polymerases, evade proofreading by viral exonucleases, and subsequently decreases viral RNA production (4). Previous studies have demonstrated that remdesivir has broad-spectrum activity against members of the filovirus (e.g., EBOV, MARV) (6), CoVs (e.g., SARS-CoV, MERS-CoV) (7, 8), and paramyxovirus (e.g., respiratory syncytial virus, Nipah virus, and Hendra virus) (9).
Remdesivir was originally developed for the treatment of EBOLA virus disease (3). Recently, in vitro studies showed that remdesivir was effective against COVID-19 in the human airway epithelial cell (10). Short term outcomes of remdesivir have been reported for 53 patients infected with COVID-19 treated in over 20 hospitals (11). It was reported that overall clinical improvement was observed in 36 of 53 patients (68%) receiving a 10-day regimen of IV remdesivir (11). However, 32 patients (60%) in the study experienced at least one adverse event, and 12 patients (23%) reported serious adverse events (11). The most common adverse events included diarrhea, rashes, septic shock, acute kidney injury, renal impairment, and hypotension (11, 12). Currently, two clinical studies are on-going to further evaluate the efficacy and safety of remdesivir for the treatment of COVID-19 respiratory disease in humans (13, 14). In one study, 308 patients with mild to moderate COVID-19 were given remdesivir as a 200 mg loading dose on day 1, then 100 mg IV once-daily for 9 days (13). In another study, the same regimen was given to 452 patients with severe clinical manifestations of COVID-19 (14).
The feasibility to deliver remdesivir via different administration routes (e.g., intravenous (IV) injection, intramuscular (IM) injection and oral administration) has been investigated (3). Unfortunately, remdesivir is not suitable for oral delivery since the drug is mostly metabolized and cleared by first-pass metabolism, resulting in poor hepatic stability and poor bioavailability (3). The delivery of remdesivir by the IM route also faces the challenge of variable release from muscle and slow acting of the active compound in peripheral blood mononuclear cells (3). Therefore, remdesivir is administrated by IV injection since this route allows wide distribution to most tissues including kidney, kidney medulla, and liver (3).
For IV administration, remdesivir was developed in two dosage forms, a concentrate solution intended for dilution and administration by infusion and a lyophilized powder for reconstitution and dilution intended for administration by infusion (3). Since remdesivir is practically insoluble in water, both formulations contain sulfobutylether-beta-cyclodextrin (SBECD) as a solubility enhancer (3). Since the excipient, SBECB, is cleared by the kidneys, remdesivir is contradicted in patients with several renal impairment (3). A pharmacokinetic study showed that both formulations are interchangeable based on similar plasma concentrations (3). Lyophilized remdesivir powder is stable when stored below 30 °C and has a shelf-life of 51 months, while remdesivir concentrate solution for dilution requires the product to be stored at freezing storage conditions (−25 °C to −10 °C) for a shelf-life of 48 months (3).
Currently, remdesivir is administered by injection into a vein as an infusion to treat patients with COVID-19 only in hospitals. However, due to the pandemic, many patients are not able to be hospitalized, and they do not have access to injectable administration of remdesivir. To provide remdesivir for other patients besides those most severely ill, more convenient and accessible dosage forms for different routes of administration must be quickly developed and tested so that patients have more options to get treated.
Intriguing strategies for future improvement of remdesivir include the development of inhaled dry powder of remdesivir for direct administration to the primary site of infection, the lungs. The mechanism of coronavirus infection is mostly in the respiratory tract, especially in the deep lungs. Hence, the inhalation route must be immediately pursued as the most promising route of administration to maximize direct delivery to the target site without first-pass metabolism, boost local antiviral activity in the lungs, and limit the potential for systemic side effects (15). In addition, the cost of the drug can be reduced, and the supplies of the drug can be maximized, thus treating more patients due to less dose required by inhalation as compared to injectable forms. The treatment cost can also be decreased when administered by inhalation, since patients may not need to visit hospitals as is required to administer the IV injectable dose. Therefore, more affordable and early stage treatment can be provided to patients with inhaled remdesivir.
Nebulization of the current IV formulation in a diluted form is a potential method of pulmonary administration; however, the drug is prone to degrade by hydrolysis in aqueous solution to form the nucleoside monophosphate, which has difficulty penetrating cell membranes, thereby minimizing the antiviral activity in the lung cells (16). Another concern is the use of sulfobutylether-beta-cyclodextrin (SBECD) as an excipient in inhalation dosage forms. Although cyclodextrin is not an excipient in an approved FDA inhaled product (17), several papers have investigated the use cyclodextrin in inhaled formulations. Tolman et al. (18, 19) previously demonstrated that aerosolized voriconazole nebulized solution that contained a diluted form of the commercially available Vfend®, an IV voriconazole dosage form containing SBECD, is capable of producing clinically relevant lung tissue and plasma concentrations of the drug in animals. However, in this form, voriconazole in lung tissue was not able to be detected 6-8 h after administration of a single inhaled dose in the animal study by Tolman et al. (18), while voriconazole dry powder lasted longer in the lungs (up to 24 h) in an animal study by Beinborn et al (20). Therefore, a dry powder formulation for inhalation can be more favorable with a smaller number of daily doses.
The advantages of dry powders for inhalation over liquids administered by nebulizers are not limited only to improve the stability of the drug during inhalation, but also dry powder inhalers provide the ease of maintenance and having a short administration time (21). The inconvenience of nebulized inhalation solutions includes the use of a large nebulizer device requiring power and water, user manipulation for cleaning and operating, and long nebulization times. Also, the cost per dose and initial cost of the nebulizer are higher than a DPI device (21). Hence, dry powder inhalation is an ideal dosage form for the treatment of COVID-19 in an outpatient setting, which would minimize the risk of spreading the virus to healthcare professionals.
Although several techniques have been used to prepare inhalable powders, including mechanical milling and spray drying, the advantages of thin film freezing (TFF) over other techniques rely on the ability to produce aerosolizable particles composed of brittle matrix, nanostructured aggregates. These are high surface area powders that are ideally suited for dry powder inhalation. TFF employs ultra-rapid freezing (on the order of 10,000 K/sec) such that precipitation (either as a crystalline nanoaggregate or amorphous solid dispersion) and particle growth of the dissolved solute can be prevented (22). Subsequently, nanostructured aggregates are formed as a low-density brittle matrix powder (23), which is efficiently sheared into respirable low-density microparticles by a dry powder inhaler upon inhalation by the patient (24). Despite a large geometric diameter (>10 microns), low-density microparticles composed of these nanostructured aggregates can be delivered to the deep lung with optimal aerodynamic diameters of <3 to 4 microns (24). Additionally, it has been reported that the engineered particles with a geometric diameter greater than 10 microns can extend drug retention time in the lungs due to the ability of the deposited particles to escape from macrophage phagocytosis (25). According to a recent study by Longest et al., computational models demonstrated that nanoaggregates are favorable for higher drug absorption efficiency and dose uniformity in the lungs, compared to microparticles (26). Furthermore, TFF can produce amorphous high surface area powders with submicron primary particles, which can enhance the dissolution rate and subsequently improve the bioavailability of poorly water-soluble drugs like remdesivir in the lungs (27).
This work aims to apply the TFF technology to develop remdesivir dry powder formulations for inhalation administered by a commercially available dry powder inhaler. We hypothesize that the ultra-rapid freezing rate of the TFF technology will produce low-density, high porosity brittle matrix powders of remdesivir, which are aerosolizable by the shear forces generated from the passive dry powder inhaler, and thus allow high doses of remdesivir to be administered to the lung.
2. Material and Methods
2.1 Materials
Remdesivir was purchased from Medkoo Biosciences (Research Triangle Park, NC, USA). Lactose monohydrate, leucine, polysorbate 20, acetonitrile (HPLC grade), and trifluoracetic acid were purchased from Fisher Scientific (Pittsburgh, PA, USA). D-Mannitol was bought from Acros Organic (Fair lawn, NJ, USA). Sulfobutylether-beta-cyclodextrin (SBECD, Captisol®) was kindly provided by CyDex Pharmaceuticals, Inc. High-resistance Monodose RS00 dry powder inhalers were kindly provided by Plastiape S.p.A. (Osnago, Italy).
2.2 Preparation of dry powder for inhalation using thin film freezing
Remdesivir and excipients (i.e., Captisol®, mannitol, lactose and leucine) were dissolved in a mixture of either acetonitrile/water (50/50 v/v) or 1,4-dioxane/water (50/50 v/v) at the solid contents shown in Table 1. The solutions were stored in the refrigerator at 2-8°C before the thin film freezing process. The solution was passed through an 18-gauge syringe needle and dropped from a height of approximately 10 cm onto a rotating cryogenically cooled stainless-steel drum. The solutions were frozen at a drum surface temperature of −100 °C. The frozen samples were collected in a stainless-steel container filled with liquid nitrogen and then transferred into a −80 °C freezer before drying in a lyophilizer. The frozen samples were primary dried at −40 °C for 20 hours, and ramped to 25 °C over 20 hours, and then secondary dried at 25 °C for 20 hours.
List of TFF remdesivir formulations and compositions.
Aerosol performance of TFF remdesivir powders using a Plastiape® RS00 high resistance DPI at a flow rate of 60 L/min (n=2). (MMAD, mass median aerodynamic diameter; GSD, geometric standard deviation; FPF, fine particle fraction; EF, emitted fraction)
2.3 Drug quantification (HPLC)
The content of remdesivir was determined through analysis with a Thermo Scientific™ Dionex™ UltiMate™ 3000 HPLC system (Thermo Scientific, Sunnyvale, CA, USA) at a wavelength of 246 nm. A Waters Xbridge C18 column (4.6 × 150 mm, 3.5 μm) (Milford, MA) was used at 30 °C and a flow rate of 0.8 mL/min. The isocratic method was performed for 4.5 minutes using a mobile phase of 50:50 (%v/v) water –acetonitrile containing 0.05% (v/v) TFA. The retention time of remdesivir was approximately ∼3.5 minutes. Dimethyl sulfloxide: acetonitrile: water (10:60:30, v/v) was used as diluent. All analyses exhibited linearity in the range tested of 0.2–250 μg/mL. All chromatography data were processed by Chromeleon Version 7.2.10 software (Thermo Scientific, Sunnyvale, CA, USA).
2.4 In vitro aerosol performance
The aerodynamic properties of the TFF powder samples were determined using a Next Generation Pharmaceutical Impactor (NGI) (MSP Corp, Shoreview, MN) connected to a High Capacity Pump (model HCP5, Copley Scientific, Nottingham, UK) and a Critical Flow Controller (model TPK 2000, Copley Scientific, Nottingham, UK). The pre-separator was not used in this study. To avoid particle bounce, the NGI collection plates were coated with 1.5% w/v polysorbate 20 in 100% methanol and then dried for 20 min before analysis. A high resistance Plastiape® RS00 inhaler (Plastiape S.p.A, Osnago, Italy) containing size #3 HPMC capsules (V-Caps® Plus, Lonza, Morristown, NJ) and 1-3 mg of powder was attached to a USP induction port by a molded silicon adapter, and the powder was dispersed to the NGI at the flow rate of 60 L/min for 4 s per each actuation. The deposited powders from the capsule, inhaler, adapter, induction port, stages 1-7, and the micro-orifice collector (MOC) were collected by diluting with a mixture of DMSO/water/acetonitrile (10:30:60 v/v). The remdesivir content in the deposited powders was determined using the HPLC method as described in Section 2.3. Copley Inhaler Testing Data Analysis Software (CITDAS) Version 3.10 (Copley Scientific, Nottingham, UK) was used to calculate the mass median aerodynamic diameter (MMAD), the geometric standard deviation (GSD), the fine particle fraction (FPF), and the emitted fraction (EF). The EF was calculated as the total amount of remdesivir emitted from the device as a percentage of total amount of remdesivir collected. The FPF of recovered dose was calculated as the total amount of remdesivir collected with an aerodynamic diameter below 5 µm as a percentage of the total amount of remdesivir collected. The FPF of delivered dose was calculated as the total amount of remdesivir collected with an aerodynamic diameter below 5 µm as a percentage of the total amount of remdesivir deposited on the adapter, the induction port, stages 1-7 and MOC.
2.5 X-ray powder diffraction (XRPD)
The crystallinity of the powders was evaluated using a benchtop X-ray diffraction instrument (Rigaku Miniflex 600 II, Woodlands, TX, USA) equipped with primary monochromated radiation (Cu K radiation source, λ = 1.54056 Å). The instrument was operated at an accelerating voltage of 40 kV at 15 mA. Samples were loaded in the sample holder and scanned in continuous mode with a step size of 0.02° over a 2θ range of 5–40 ° at a scan speed of 2 °/min, and a dwell time of 2 s.
2.6 Modulated differential scanning calorimetry (mDSC)
Thermal analysis of powder samples was conducted using a differential scanning calorimeter Model Q20 (TA Instruments, New Castle, DE) equipped with a refrigerated cooling system (RCS40, TA Instruments, New Castle, DE). Samples of 1-3 mg were weighed and loaded into a T-zero pan. The pan with a T-zero hermetic lid were crimped, and a hole was drilled in the lid before placing the pan in the sample holder. To evaluate the glass transition and glass forming ability type of remdesivir unprocessed powder, samples were heat at a heating ramp rate of 10 °C/min from 25 °C to 150 °C, then cooled down to −40 °C, and then heated again to 250 °C. To investigate crystallinity of the TFF formulations, samples were heated from 25 °C to 350 °C with a heating ramp rate of 5 °C/min. The scans were performed with a modulation period of 60 s and a modulated amplitude of 1 °C. Dry nitrogen gas at a flow rate of 50 mL/min was used to purge the DSC cell throughout the analysis. Data were processed by TA Universal Analysis 2000 software.
2.7 Scanning electron microscopy (SEM)
Scanning electron microscopy (Zeiss Supra 40 C SEM, Carl Zeiss, Heidenheim an der Brenz, Germany) was used to identify surface particle morphology of the TFF remdesivir powder formulations. A small amount from each of the powder formulations was placed on a carbon tape. A sputter coater was used to coat all samples with 15 nm of 60/40 Pd/Pt before capturing the images.
2.8 Nuclear Magnetic Resonance (NMR)
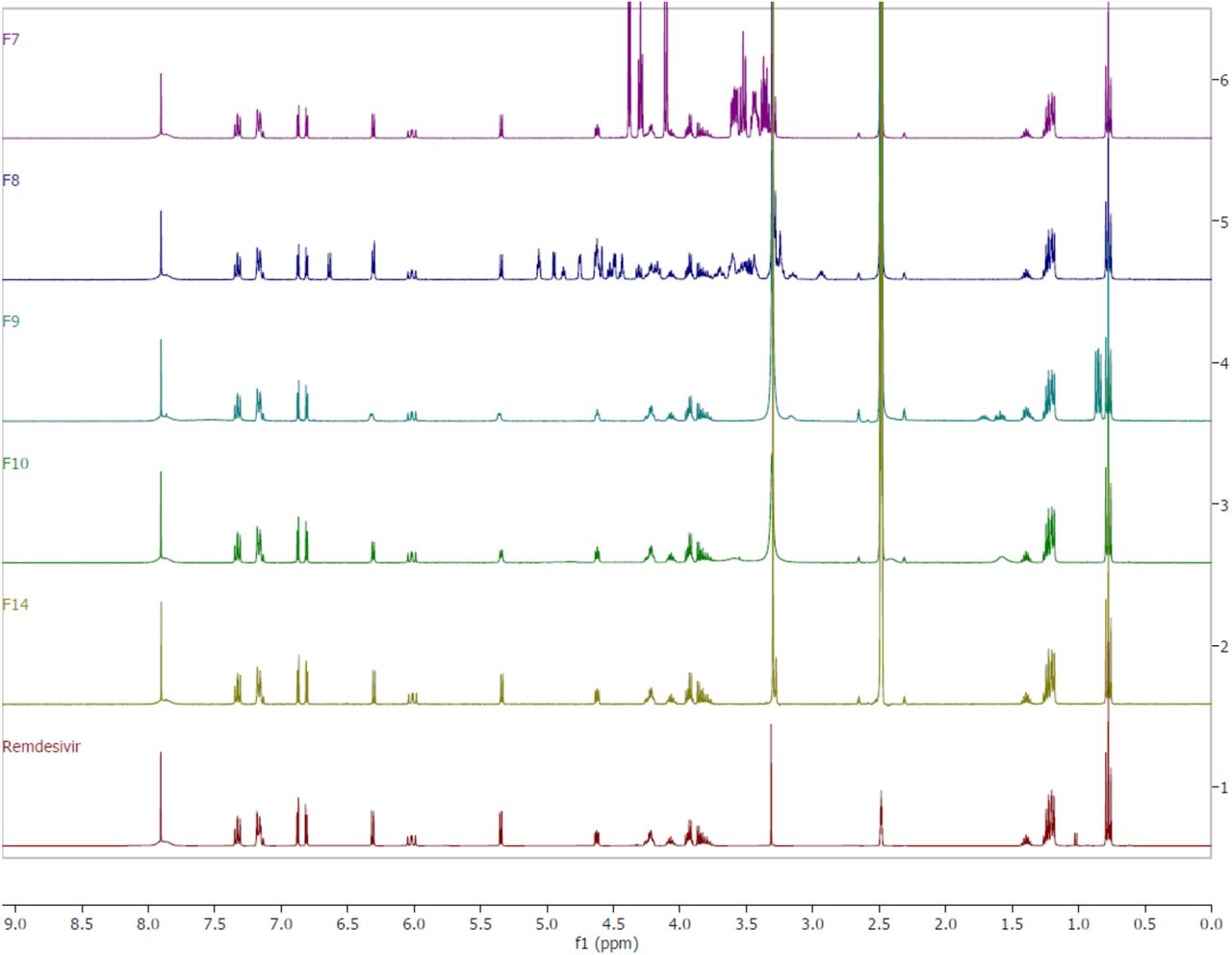
1H-NMR spectra were obtained using a Varian® NMR 400 MHz Spectrometer (Agilent Inc., Palo Alto, CA, USA) at 25 °C and were used to confirm the purity of remdesivir in the TFF powders. Formulations F7, F8, F9, F10, F14 and remdesivir drug substance were dissolved in dimethyl sulfoxide- d6 (DMSO-d6). Solutions were then transferred to 5 mm NMR tubes for NMR data acquisition. Chemical shifts were referenced to a residual solvent, DMSO, at 2.48 ppm. The NMR spectrum peaks of remdesivir in the formulations produced by TFF were compared to those of remdesivir unprocessed powder as received from the vendor.
3. Results
3.1 Physical properties of TFF remdesivir
The particle morphology of TFF remdesivir powder formulations containing different drug loadings and different excipients was determined using SEM. All formulations exhibited a brittle matrix structure of highly porous particles (Figure 1). At the same drug loading, Captisol®- and leucine-based formulations showed relatively smaller nanostructure aggregates, compared to mannitol- and lactose-based formulations. For 100% drug processed by TFF, different cosolvent systems resulted in different particle morphologies. A mixture of 1,4-dioxane/water produced smaller nanostructure aggregates, compared to a mixture of acetonitrile/water.

Figure 2 shows the x-ray diffraction patterns of TFF remdesivir powder formulations. No sharp peaks of remdesivir were observed in any of formulations indicating remdesivir was amorphous after the TFF process. The drug loading and type of cosolvent did not affect the morphology of remdesivir. For excipients, sharp peaks of mannitol were observed in F3 and F7, indicating that mannitol in these formulations remained crystalline (d-mannitol), while Captisol®, lactose, and leucine were amorphous after the TFF process.

mDSC was employed to identify the glass-forming ability of remdesivir and determine the glass transition temperature (Tg) of remdesivir. Figure 3A shows a mDSC thermogram of remdesivir unprocessed powder. The first heating cycle demonstrated remdesivir was crystalline with a melting point of ∼127 °C. The cooling and second heating cycle showed that the glass transition temperature of remdesivir was about 60 °C. No recrystallization peak was observed in any cycle.

Figure 3B shows the physical state of remdesivir and excipients. Despite the different formulation compositions, no melting peak of remdesivir was observed in any formulation. These results agree with XRD diffractograms showing that remdesivir was amorphous after the TFF process. The mDSC thermogram shows that the Tg of remdesivir in all formulations was in the range 58-61 °C.
3.2 Chemical stability of TFF remdesivir
Chemical stability of remdesivir after TFF processing was confirmed by 1H-NMR. Figure 4 presents the 1H-NMR spectra of selected TFF remdesivir powder formulations and remdesivir unprocessed powder. Remdesivir peaks from the TFF remdesivir powder formulations consisting of 50% (w/w) remdesivir with mannitol, lactose, and leucine (F7, F8, and F9, respectively) are identical to the peaks of remdesivir unprocessed powder. The 80% (w/w) of remdesivir with Captisol® (F10) and 100% remdesivir without excipient (F14) also presented indistinguishable peaks corresponding to remdesivir. Therefore, neither the aqueous-organic cosolvent mixture nor the conditions used in the TFF process affected the chemical stability of remdesivir.


3.3 Aerodynamic properties of TFF remdesivir
The aerodynamic particle size distribution of TFF remdesivir formulations was evaluated using a Plastiape® RS00 high resistance DPI and NGI apparatus. In vitro aerodynamic testing revealed that drug loading affected the aerosol performance of the TFF formulations. Despite using different excipients, the aerosol performance generally increased as the drug loading was increased. The FPF (of recovered dose) of Captisol®-based formulations containing 5%, 20%, 50% and 80% of remdesivir (F1, F2, F6, F10, respectively) were 30.22%, 42.79%, 64.73% and 68.29%, respectively. The MMAD of these TFF remdesivir powder formulations was 3.12 µm, 2.67 µm, 2.30 µm, and 2.28 µm, respectively. For lactose- and mannitol-based formulations, there were significant increases in FPF (of recovered dose) when the drug loading was increased from 20% to 50%; however, FPF did not significantly change when the drug loading was increased further from 50% to 80% with these materials. Interestingly, FPFs of leucine-based formulations containing 20%, 50% and 80% of remdesivir were not significantly different. However, MMADs of these leucine-based formulations at drug loadings of 20%, 50% and 80% increased from 0.77 µm to 0.86 µm to 1.46 µm, respectively. When the drug loading was increased to 100% (i.e., excipient free), F14 exhibited an FPF of 62.33% (of recovered drug) and an MMAD of 2.06 µm.
An effect of the excipient on aerosol performance was also observed. At the same drug loading, leucine-based formulations exhibited significantly greater FPF (81-85% FPF), and smaller MMAD (0.8− 1.5 µm), compared to other excipients, which indicates that leucine has advantages over others in terms of aerosol performance.
We also investigated the effect of cosolvent mixture on the aerosol performance of the formulations. For 100% drug loading, significant differences in MMAD, FPF, and EF were observed between the formulations using acetonitrile/water and 1,4-dioxane/water (F14 and F15, respectively). F15 exhibited smaller MMAD, larger FPF and EF compared to F14.
4. Discussion
4.1 Thin film freezing can produce high potency remdesivir dry powders for inhalation with high aerosol performance
We investigated the feasibility of thin film freezing to prepare inhalable remdesivir powder formulations. Different excipients including Captisol®, mannitol, lactose, and leucine were selected in this study. Mannitol and lactose are presently contained in FDA approved inhalation dosage forms, while leucine has gained more interest for pulmonary delivery. Captisol® was selected in this study since it is a solubilizer used in both the solution concentrate for dilution and infusion and the lyophilized powder for reconstitution/dilution and infusion (3).
The RS00 high resistance monodose DPI is a capsule-based DPI device that is available for commercial product development, and it functions to disperse powder based on impaction force. A previous study confirms that this impact-based DPI can disperse low-density brittle matrix powder made by TFF into respirable particles better than a shear-based DPI (e.g., Handihaler®) (28). Another study also evaluated the performance of different models of monodose DPI (RS01 and RS00) on the aerosol performance of brittle matrix powders containing voriconazole nanoaggregates prepared by TFF (29). It was shown that the RS00 device exhibited better powder shearing and deaggregation through smaller holes of the capsule created by the piercing system of the RS00 device (29). Therefore, the RS00 high resistance Plastiape® DPI was selected in this study.
We found that excipient type and drug loading affect the aerosol performance of TFF remdesivir. Overall, the aerosol performance of TFF remdesivir powders increased as the drug loading was increased. This trend is obvious for the Captisol®-, lactose-, and mannitol-based formulations when the drug loading was increased from 20% to 50%. Furthermore, high potency TFF remdesivir powder without excipients (F14 and F15) also exhibited high FPF and small MMAD, which indicates remdesivir itself has a good dispersing ability without the need of a dispersing aid when prepared using the TFF process. This shows the TFF technology can be used to minimize the need of excipient(s) in the formulation, thus maximizing the amount of remdesivir being delivered by dry powder inhalation.
Although the aerosol performance of leucine-based formulations did not significantly change when the drug loading was increased from 20% to 80%, these formulations exhibited superior aerosol performance compared to other excipient-based formulations. This is likely attributed to the surface modifying properties of leucine. Several papers report that leucine can minimize the contact area and distance between particles (30, 31). This decreases Van der Waal forces between drug particles and subsequently increases aerosol performance.
Additionally, different cosolvent systems affected the aerosol performance of TFF remdesivir powders. The formulation prepared in a 1,4-dioxane/water cosolvent system (F15) exhibited smaller MMAD and higher FPF than the formulation prepared in an acetonitrile/water cosolvent system (F14). This agrees with SEM figures showing that F15 has smaller nanostructured aggregates than F14. This is possibly due to the difference in viscosity of the solvent. The viscosity of ACN/water (50/50 v/v) was lower than that of 1,4-dioxane/water (50/50 v/v) (0.81 vs. 1.62 mPa·s) (32, 33). Our results agree with the previous studies by Beinborn et al. (34) and Moon et al. (29) showing that the viscosity of the solvent system has an impact on the aerosol performance of TFF powder. The higher viscosity of the cosolvent minimizes the movement of molecules during the ultra-rapid freezing step, resulting in more homogenous distribution in the frozen state (29). On the contrary, the lower-viscosity solvent allows molecules to move more easily, which increases the chance of molecular aggregation and subsequently decreases the aerosol performance (29).
4.2 Physical and chemical stability of remdesivir dry powder produced using TFF
Both XRD diffractograms and DSC thermograms showed that remdesivir was amorphous after the TFF process. An amorphous form of the drug generally provides for faster dissolution rate than its crystalline form. Since the drug needs to be absorbed and then penetrate through the cell membrane before it is hydrolyzed to nucleoside monophosphate, TFF remdesivir powders may provide benefits for the dissolution of the deposited powder in the lung fluid that leads to improvement in the bioavailability and efficacy of the drug when administered by inhalation.
One concern related to the amorphous drug is physical instability due to its high energy state. According to criteria described in Wyttenbach et al., our study confirmed that remdesivir is categorized as a class III glass-forming drug (i.e., it is a stable glass former) (35), because no crystallization peak was observed in both the cooling and heating cycles on DSC. This provides evidence that TFF remdesivir can maintain its physical stability during storage.
In addition to the physical stability, remdesivir, as a prodrug, is prone to degrade by hydrolysis in aqueous solution. Since an organic/water cosolvent system is required to dissolve the drug and excipients in the TFF process, chemical stability is another concern during preparation. NMR spectra demonstrated that remdesivir did not chemically degrade as a result of the TFF process. Even though remdesivir was exposed to binary solvent systems consisting of water during the process, the entire TFF process used to produce remdesivir dry powder inhalation formulations did not induce chemical degradation of the parent prodrug.
5. Conclusions
We have demonstrated that low density, highly porous brittle matrix particles of remdesivir powder formulations made by thin film freezing are highly aerosolizable and suitable for inhaled delivery. The properties of a good glass former, like remdesivir, provide evidence that the physical stability of the remdesivir contained in the dry powder formulations should not change during storage if protected from moisture. The thin film freezing process is suitable to prepare remdesivir dry powder for inhalation without causing chemical degradation. Therefore, remdesivir dry powder for inhalation produced using thin film freezing technology is being pursued as a promising dry powder inhalation product to provide therapy for the treatment of patients with COVID-19.
Acknowledgement
Moon, Sahakijpijarn and Williams acknowledge TFF Pharmaceuticals, Inc. for the financial support through a sponsored research agreement. All authors are co-inventors on related intellectual property. The Board of Regents of The University of Texas has licensed IP covering inhaled remdesivir formulations prepared with thin film freezing to TFF Pharmaceuticals, Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}