

Abstract
Evaluating correctly others’ pain is a crucial prosocial ability, especially relevant for the healthcare system. In clinical settings, caregivers assess their patients’ pain under high workload and fatigue, often while dealing with competing information/tasks. However, the effect played by such cognitive strain in the appraisal of others’ pain remains unclear. Following embodied accounts that posit a shared representational code between self and others’ states, it could be hypothesized that the representation of people’s pain might be influenced by cognitive exertion similarly to first-hand experiences.
Fifty participants underwent one of two demanding tasks, involving either working memory (Experiment 1: N-Back task) or cognitive interference (Experiment 2: Stroop task). After each task, participants were exposed to painful laser stimulations at three intensity levels (low, medium, high), or video-clips of patients experiencing three intensity levels of pain (low, medium, high). Participants rated the intensity of each pain event on a visual analogue scale.
We found that the two tasks influenced rating of both one’s own and others’ pain, by decreasing the sensitivity to medium and high events. This was observed either when comparing the demanding condition to a control (Stroop), or when modelling linearly the difficulty/performance of each depleting task (N-Back). These effects were mirrored by the analysis of physiological responses (Heart Variability and Skin Conductance) evoked by one’s own pain.
We provide converging evidence that cognitive exertion affects the subsequent appraisal of one’s own and likewise others’ pain. Healthcare personnel should be aware that high workload might alter their cognitive abilities.
Introduction
Identifying and assessing the intensity of pain experienced by others is a crucial ability, especially in clinical settings1–5. Unfortunately, physicians and nurses are often subject to long/irregular work shifts, fatigue and poor sleep that may overload of their cognitive resources. However, it is still unclear how such extensive mental exhaustion might interfere with their clinical abilities, in particular the assessment of others’ pain.
Previous studies converge in finding that depletion of individual cognitive resources led to a generally reduced sensitivity to concurrent own pain experience6–9. However, it is less clear whether similar influence linger also after the task completion. For instance, being engaged in a highly demanding Stroop task decreased the sensitivity to subsequent intense stimulations in a study10, but it increased the sensitivity to mild noxious events in others11,12. Such mixed findings beg for a systematic investigation of after-effects of cognitive exertion on pain, to account also for concerns about reliability of such paradigm which have recently been put forward by the research community13,14.
Most critically, it is unclear whether cognitive exertion would impact the assessment of pain of others similarly to one’s own. Seminal models from social psychology/neuroscience suggest that others’ suffering is partially processed in an embodied fashion, i.e. by recruiting the same mechanisms underlying one’s own first-hand experiences15–19. Indeed, analgesic manipulations (e.g., acetaminophen, hypnosis, placebo) can similarly influence the sensitivity to self and others’ pain20–22. Furthermore, neuroimaging studies suggest that self and others’ pain share a partly-common neuronal representation in a widespread network including the middle cingulate cortex20,23,24, a brain region held to play a key role in the regulation of one’s pain responses12,25 (but see26). Hence, it is reasonable to assume that such regulatory mechanisms might equally impact the representation of one’s and others’ pain.
An alternative model, the broaden-and-build theory, suggests instead that positive emotions/mood can broaden one’s resources, improving physical, intellectual and social abilities, whereas negative emotions would narrow one’s resources, thus promoting self-related thoughts27. Consistently, previous studies showed that negative events cause hyperalgesia28,29,38,39,30–37, but have opposite effects for the pain of others by decreasing physiological and neural response to the sight of people’s injuries33. Importantly, the broaden-and-build explains these effects in terms of an indirect modulation of emotions on one’s cognitive resources27. Consequently, narrowing one’s resources through other means (e.g., cognitive exertion) should lead to the same effects, by increasing the sensitivity to self-pain (as found by11,12) at the expense of sensitivity to other people’s pain.
Here we engaged participants in one of two demanding paradigms, involving either working memory (Experiment 1: N-Back task) or inhibition (Experiment 2: Stroop task), to investigate the effects of cognitive exertion on the subsequent assessment of one’s and others’ pain. Based on previous research, we expected the demanding tasks to influence sensitivity to self-pain (albeit with unascertained direction10,11,12). The critical question was whether the same manipulation would influence the pain perceived in others in similar (as predicted by embodied accounts) or opposite fashion (broaden-and-build) with respect to self-experienced pain.
Methods
Participants
Recruitment took place through advertisements posted at the University of Geneva buildings and online platforms. We excluded from our experiment all individuals with the following characteristics: history of substance/alcohol abuse, history of neurological or psychiatric illness, fever or an ongoing acute medical condition and extreme dark skin colour (because radiation absorption of dark skin is higher for the wavelength of the laser device used for nociceptive stimulations40,41). They declared good health and typical cognitive proficiency, they had good (or corrected) visual acuity. In addition, as Experiment 2 involved verbal material, we included only French native speakers. Based on these criteria, we recruited a total of 75 participants, sixteen of which were subsequently excluded due to falling asleep during data acquisition (one participant) or lack of sensitivity to the nociceptive stimulation (15 participants). The latter criterion was established in those participants who, during the main experiment, rated the highest stimulation under the control condition < 4 on a 10-points pain intensity scale (see below for more details), despite good sensitivity to pain during a preliminary calibration phase. We further excluded 9 participants who were not susceptible to the task manipulation. This was achieved by calculating a combined index for accuracy and response time (Inverse Efficiency Score42,43) during the task, and by removing those participants whose performance in the difficult (demanding) condition was comparable/better than in the control condition (see Results section and Figure 2).
This led to a final sample of 50 participants: 25 took part in Experiment 1 (14 females; aged 19 to 37, Mean = 25.16, SD = 5.03 years) and 25 individuals in Experiment 2 (14 females; aged 18 to 36, Mean =23.52, SD = 4.28 years). Sample size was consistent with the previous studies on which the present research is based11,44. Participants were all naïve to the purpose of the study and none of them participated in both experiments. This study was approved by the local ethical committee (Commission Cantonale d’Éthique de la Recherche of Geneva, protocol code: CCER N. 2019-01355) and conducted according to the Declaration of Helsinki.
Measures
Nociceptive stimulation
Nociceptive radiant heat stimuli was delivered by an infrared neodymium: yttrium-aluminum-perovskite laser system (Neodinium: Yttrium Aluminium Perovskite; Stimul 1340 El.En®; wavelength 1.34 μm; pulse duration 4 ms, beam diameter 6 mm2). At this short wavelength, the skin is highly transparent to laser stimulation, and consequently, the laser pulses directly and selectively activate Aδand C fibers nociceptive terminals located in the superficial layers of the skin45,46. Since these fibers have different conduction velocity, participants experienced a double sensation: an initial pricking pain due to Aδ-fiber stimulation, followed by a C-fiber-related burning pain. Laser pulse was transmitted through an optic fiber of 10-meter length, with a diameter of 6 mm by focusing lenses. Laser beam was directed to a rectangular skin area (approximately 4 × 2 cm, main axis mediolateral) on the back of the non-dominant hand. To avoid receptor sensitization, as well as damages from long-term exposure, the laser beam was relocated after each trial within a predefined stimulated skin area (see also 47).
Stimuli for Other-Pain condition
To assess the ability to recognize pain in others, we used stimuli taken from a database of videos of patients faces, some of which had spontaneous (non-simulated) expressions of pain48. Thirty videos were cut to last 3 seconds and to show the most salient expressions. For video piloting, 21 independent participants rated these short videos online (14 women; age 22 to 35, Mean = 27.6, SD = 4.7). For the purpose of this experiment, we selected 24 videos based on median ratings of the piloting that could match the three levels of self-pain (8 videos per each level of pain), one characterized by low (L), one characterized by medium (M) and one characterized by high (H) level of painful expression corresponding to about 2, 4 and 6 on the pain intensity scale. Furthermore, as the people depicted in the videos were also probed to rate their own pain experience48, we could thus check that the videos for the three levels of other’s pain exhibited clear-cut differences in low, medium and high self-reported pain. This insured that the selected clips clearly depicted three distinct intensity levels from both the point of view of the video-recorded people, and from an independent sample of observers.
Judgment ratings
Participants rated each pain stimulation using two scales (for both pain conditions, self and other): (i) a pain intensity scale to evaluate the level of pain experienced, and (ii) a pain metacognition scale to express participants’ confidence about their preceding rating on the pain intensity scale. When a scale appeared on the screen, a light blue cursor was always present in a random position on the line. Participants could move this cursor along the scale pressing buttons of a response box, one to go on the left, another to go on the right and a third button to confirm their choice.
Pain Intensity scale
Participants rated pain on a 10-point visual analogue scale ranging from not at all painful (0) to worst pain imaginable (10). This scale is a unidimensional method to assess painful experiences and is largely used by clinicians and researchers49. In the present study, it was used to rate both pain conditions, judgments of participants’ own physical pain and their judgments of others’ painful expressions. Extreme manikins of the arousal scale of the Self-Assessment Manikin (SAM) were displayed at the extremities of the scale for assessing pain intensity as an economical and straightforward cue50. Only for the self-pain calibration session (see below), we included numbers under the rating line, coloured from green (0) to red (10), to visually help participants choosing their answer.
Pain Metacognition scale
To investigate pain decision-making process, we administered a pain metacognition scale after each pain intensity rating. In both pain conditions, participants had to express their confidence about their previous pain judgment on a 10-point visual analogue scale ranging from no confidence at all (0) to completely confident (10). Extreme manikins of the dominance scale of the Self-Assessment Manikin (SAM) were included at the extremities of the metacognition scale50.
Questionnaires’ battery
In addition to the general information sheet (including questions about sex, age and hand dominance), participants filled out the Pain Catastrophizing Scale51 (PCS) and the Interpersonal Reactivity Index52 (IRI), because we hypothesized that these dimensions of personality might modulate the effects of interests. In the PCS, participants were asked to indicate the degree to which they think and feel when they experience pain using a 0 (not at all) to 4 (all the time) scale. A total score is yielded (ranging from 0-52), along with three subscale scores assessing rumination, helplessness and magnification, which respectively report rumination about pain (e.g. “I can’t stop thinking about how much it hurts”), feeling helpless to manage pain (e.g. “There is nothing I can do to reduce the intensity of my pain”) and magnification of pain (e.g. “I’m afraid that something serious might happen”).
The IRI measures various aspects of empathy including cognitive and emotional empathy. Participants had to answer 28 statements using a 5-point scale, ranging from “Does not describe me well” to “Describes me very well”. This measure is divided in four seven-item subscales. The perspective taking (PT) scale reports tendency to spontaneously adopt the psychological point of view of others in daily life (e.g. “I sometimes try to understand my friends better by imagining how things look from their perspective”). The empathic concern (EC) scale assesses the tendency to experience feelings of sympathy and compassion for unfortunate others (e.g. “I often have tender, concerned feelings for people less fortunate than me”). The personal distress (PD) scale taps the tendency to experience distress and discomfort in response to extreme distress in others (e.g. “Being in a tense emotional situation scares me”). The fantasy (FS) scale measures the tendency to imaginatively transpose oneself into fictional situations (e.g. “When I am reading an interesting story or novel, I imagine how I would feel if the events in the story were happening to me”).
General experimental procedure
To disentangle the opposing theoretical predictions concerning the impact of exertion on others’ pain judgment (see Introduction section), we systematically modulated work load (factor Load: low vs high), type of pain (factor Type: self vs other) and pain intensity (factor Intensity: low, medium, high). In this study, volunteers assessed their pain sensitivity and judgments of others’ pain after a low or high cognitive demanding task in two experiment (N-Back in Experiment 1 and Stroop in Experiment 2). These two experiments followed the same procedure. On arrival, participants read carefully and signed the informed written consent, then they were reminded that each laser stimulus would be very fast (only 4 ms) and that they could ask to stop the experiment at any time. All tasks and stimuli were coded, managed and presented with Psychophysics Toolbox Version 3 (PTB-3, http://psychtoolbox.org/), a free set of Matlab R2018b (Mathworks, Natick, MA). The experimental session consisted of two parts: 1) pre-test divided in pain thresholding session and training of the task, and 2) main experiment divided in two experimental sessions. Participants had to use a response box with four buttons in their dominant hand to answer. Two experimenters were always present during the experimental session. One experimenter was responsible for technical checks of the equipment before and during acquisition, including physiological measures, laser inputs and behavioural recordings. The other experimenter was responsible for interacting with participants and delivering painful stimulations by directing the laser beam on participants’ hand. Importantly, the latter experimenter was unaware of the level of pain emitted by the laser.
To insure protection from adverse effects of the laser, the following procedure were put in place. The experiment was carried out in an ad hoc room, protected with laser safety curtains certified for the wavelength of the stimulator. Furthermore, participants and experimenters wore eye-protection goggles with optical density ≥ 2 at 1.34 μm. Participants were asked to remove all accessories from their non-dominant hand to allow safe stimulation of the skin area.
As described above, pain stimulus intensity was individually calibrated for each participant based on a random staircase thresholding session53 to determine stimulations eliciting three levels of pain that were then used in the main experiment. Each trial started with a flash appearing on the screen for 3 seconds indicating that the stimulation was about to come, while the laser was preparing to deliver the correct amount of energy. After each stimulation, participants answered on the pain scale (with no time restriction). The calibration session lasted about 15 minutes. At the end of this session, we obtained a pain curve based on which we would then select three different energies that corresponded to three different levels of pain for each participant (medians of about 2, 4 and 6 on the pain rating scale) for low (L), medium (M) and high (H) self-pain.
After the pain calibration, a training session was administered which was divided in two parts. First, participants were trained to perform the N-Back task in Experiment 1 or the Stroop task in Experiment 2. Then, in the second part of the training, participants watched three videos displaying patients with low level of pain based on the piloting session. These videos were taken from the same database, but not included in the main experiment. Participants had to judge pain intensity and confidence about their pain judgment.
During main experiment, we recorded physiological responses to stimuli from their left hand, such as skin conductance (EDA) and heart rate. These physiological measures were acquired using the Biopac System and Acknowledge software. Electrodermal activity was recorded from two disposable GSR/EDA electrodes (EL507, Neurospec AG) placed on the middle and ring fingers, while cardiac pulse was recorded placing a transducer on the index finger (Biopac System). In the main experiment, each participant performed four blocks representing the experimental condition (cognitive exertion) and four blocks of a neutral (baseline) condition, presented in a pseudorandom order Error! Reference source not found.. Each block was further divided in two parts. In the first part, participants performed the task, N-Back (Exp. 1) or Stroop (Exp. 2), for about two minutes, followed in the second part by the delivery of six stimulation-trials in random order. In “Self” blocks, these were characterized by 2 Low, 2 Medium and 2 High pain stimulations. Each trial started with a flash appearing on the screen for 3 seconds indicating that a stimulation was about to come. In “Other” blocks, three different level of pain expressions (corresponding to Low, Medium, and High) were used and each video lasted 3 seconds. For each trial of either Self or Other condition, the pain stimulus was followed by a black screen lasting for 1 second and then the visual analogue scale for pain judgement appeared on the screen, prompting participants to evaluate the level of felt (for “Self”) or inferred (for “Other”) pain (5 seconds duration). After 1 second of black screen, the visual analogue scale for confidence judgement appeared on the screen (5 seconds duration). Then, a black screen appeared for a random inter-trial interval ranging between 2.5 and 4.5 seconds with steps of 200 ms. Overall each block lasted about 3 minutes. Overall, the experiment session lasted 1 hour and half and, at the end, participants were refunded for their time and effort (30 CHF).
N-Back task
In Experiment 1, we administered an N-Back task54, which was previously used successfully to evaluate the impact of distraction on pain sensitivity44. Participants monitored a series of stimuli appearing one at a time on the screen. They were required to identify if the stimulus presented was the same as the one presented n previous items by pressing one button (‘yes’) and if not by pressing a different button (‘no’). In the current study, n was set to be 3 (high cognitive load condition) or 0 (low cognitive load condition). In the 3-Back condition, participants were required to constantly update the target letter, by retrieving from working memory the one letter occurring 3 items before. For instance, if we pretend a sequence of letters “RGSR”, correct answer to the last would be “yes”, as the same letter occurred also three trials before in the sequence “RSGP” but in this case answer is “no”. As control, we implemented a low cognitive load condition, in which participants were asked to respond only on the trial that they were currently processing, by pressing “yes” whenever a predefined stimulus (“V” letter) would be presented. In each block, a total of 18 letter stimuli were presented one at a time with 4 target-hits.
Each letter was presented for 500 ms, followed by an inter-trial interval (ITI). The ITI between letters of the 0-Back condition was fixed at 700 ms. Instead, for the 3-Back condition to reduce within-participant variation, the ITI was considered as a measure to calibrate task difficulty and the mean ITI was adapted based on participants’ performance in the previous block (i.e., corresponding to 18 previous trials). This is roughly comparable to a previous study with a similar design (adaptation based on previous 15 trials44), although in that case, the authors tested pain concurrently to the N-Back, and therefore had no need to divide the experimental session into small blocks44. Target sensitivity was assessed with the non-parametric signal detection measure A’ 55,56. This parameter is computed from a pair of hit and false alarm rates44: a value near 1 indicates a good discriminability, whereas a value near 0.5 (when hits are equal to false alarm) indicates chance performance. Initial duration of the empty screen was 700 ms. Then based on the previous trial, when discriminability was higher than the targeted level of A’ = .75, empty screen interval was reduced, while with a discriminability lower than A’ = .75 it was increased.
During the training session, the order of the blocks was fixed: the first block was 0-Back, the second block was 3-Back in which subsequent adjustments were made after each trial. Instead, in the main experiment, the order of blocks was pseudorandomized and difficulty of the task was calibrated by adapting the interval for each participants’ performance to the previous 3-Back block. Thirteen participants (7 women) started with two blocks 0-Back condition (low cognitive load) and then two blocks with high cognitive load (combined with 2 “Self” and 2 “Other” in a pseudorandomized order) followed by a break of about 5 minutes and then the same task sequence was repeated (combined with 2 “Self” and 2 “Other” in a pseudorandomized order). With the same procedure, twelve participants (7 women) started with the 3-Back condition (high cognitive load).
Stroop task
In Experiment 2, we administered the Stroop task, which was already previously found having an after-effect on self-pain11. Each participant performed neutral and interference conditions of the numerical Stroop task57. Participants were informed that they would see sets of one to four identical words presented vertically on the screen. They were asked to count how many times a word was presented on the screen using buttons of the response box as quickly and accurately as possible, with a strong emphasis placed on not sacrificing accuracy for speed. Moreover, participants were asked not to use strategies to make the task easier (like blur words on the screen). In the interference condition, words stimuli were number words ‘one’, ‘two’, ‘three’ and ‘four’ – presented in French (‘un’, ‘deux’, ‘trois’, ‘quatre’) and they were always incongruent stimuli (word meaning and number of repetitions were different). In the neutral condition, words stimuli were neutral words matched in length with the number words: ‘an’, ‘drap’, ‘table’ and ‘quille’, corresponding in English to ‘year’, ‘sheet’, ‘table’ and ‘skittle’. All words were presented in capital letters. Trials started with a fixation cross (1000 ms) followed by a display with words to count which stayed on the screen until participants gave their response but no more than 1250 ms.
During 18 practice trials with neutral condition, participants received correctness feedback and were also informed to answer more quickly if they did not provide an answer within the allotted time. Feedback appeared for 2500 ms. To control for order effects, in the main experiment, half of the participants (n = 13, 6 women) had first four blocks with neutral condition (2 “Self” and 2 “Other” in pseudorandomized order), followed by a break of about 5 minutes and then four blocks with interference condition (2 “Self” and 2 “Other” in pseudorandomized order). Half of the participants instead had the interference condition first (n = 12, 9 women).
Data processing
Behavioral Measures
We first checked that participants were susceptible to the main task (Exp 1: N-Back; Exp 2: Stroop). To this purpose, we considered all participants who displayed good sensitivity to pain and complied with the experiment (Exp 1: N = 26, Exp 2: N = 33; see Participants subsection). In this analysis, trials with reaction times < 100 ms were removed as potentially reflective anticipatory response unrelated to the task. For each participant, each task and each condition, we calculated the average accuracy, median reaction times of correct responses, and combined Inverse Efficiency Score (IES),  . After acquisition, all these measures were fed to a paired-sample t-test assessing effects of task difficulty (Exp 1: N-Back 3 vs. 0; Exp 2: Interference vs. control). Then, individual data were used to exclude from all subsequent analyses those participants who were not susceptible to the task (final sample: Exp 1: N = 25, Exp 2: N = 25; see Results and Figure 2).
. After acquisition, all these measures were fed to a paired-sample t-test assessing effects of task difficulty (Exp 1: N-Back 3 vs. 0; Exp 2: Interference vs. control). Then, individual data were used to exclude from all subsequent analyses those participants who were not susceptible to the task (final sample: Exp 1: N = 25, Exp 2: N = 25; see Results and Figure 2).
To test for the effect of the task (N-Back or Stroop) on the subsequent pain experience, pain intensity and confidence ratings of each session were fed to the predictors of interest through a linear mixed model with task condition (control vs experimental) and intensity of pain (low, medium, high) as fixed factors. The subject’s identity was modelled as random factor, with random intercept and slope for the two fixed factors and the interaction therefor. Specifically, we ran two models, one for the Self-Pain condition, and the second for the Other-pain conditions. Significance associated with the fixed effects was calculated with a Type III Analysis of Variance using the Satterthwaite approximation of the degrees of freedom, as implemented in the lmerTest package58 of R (https://cran.r-project.org/) software.
Physiologic Responses
Pain elicits several physiologic responses, including skin conductance and heart rate59. In this study, these measures were monitored and collected to investigate and elucidate possible mechanisms underlying the relationship between cognitive fatigue and pain judgments.
Skin conductance
Electrodermal activity data were first subjected to a low-pass filter (cut-off frequency: 5Hz) to account for movement-related artefacts. The filtered signal was then processed and analysed with Ledalab60, a free Matlab-based toolbox. More specifically, the time course was down sampled to 50 Hz, smoothed (adaptive Gaussian), and visually inspected for potential remaining movement artefacts, which were corrected through spline interpolation. The resulting signal was then de-convolved using continuous decomposition analysis, which separates traces into tonic (slowly changing skin conductance level) and phasic (rapidly changing response) activity components. For the purpose of this analysis, we considered as reliable skin conductance response (SCR), a cumulative increase of phasic activity occurring between 1 and 5 s from the painful event (either on one’s body or through video) and exceeding 0.01 μS. These single trial estimates of SCR were square-root transformed to improve compliance with normal distribution and fed to the same statistical pipeline used for the analysis of the behavioural measures.
Cardiac response
As for pulse, cardiac response was band-pass filtered (between 10–30Hz), electrocardiographic R waves were detected offline, and intervals between heartbeats were used to estimate Heart Rate Variability (HRV) over a time-window of 14 seconds from the onset of the painful stimulation/video. More specifically, we calculated single trial estimates of the Root-Mean-Squared Sequential Difference (RMSSD)61, which is a measure used to quantify the amount of HRV observed during monitoring periods that generally may range from <1 min to >24 h. HRV and its indices like the RMSSD have been shown to be reliable indexes of physiologic response to pain62 and they have been proposed as measures of cognitive fatigue and self-regulatory strength63,64. This time-window was chosen as it captures modulations associated with painful events and ratings, without never exceeding the onset of the subsequent trial. RMSSD measures were then fed to the same analytical pipeline used for the other measures.
Results
Task Demands
We first assessed whether participants exhibited higher difficulty in the demanding conditions (Exp. 1: N-Back 3 vs. 0; Exp. 2: Interference vs. Control). We focused on all participants who displayed adequate sensitivity to pain (Exp. 1: N = 26, Exp. 2: N = 33; see Methods) and found that, on average, they displayed significant differences across the two conditions of interest in accuracy (Exp. 1: t(25) = 8.64, p < 0.001; Exp. 2: t(32) = 1.19, p = n.s.), reaction times of correct responses (Exp. 1: t(25) = 5.45, p < 0.001; Exp. 2: t(32) = 5.53, p < 0.001), and combined inverse efficiency score (Exp. 1: t(25) = -5.83, p < 0.001; Exp. 2: t(32) = -4.41, p < 0.001). However, although the tasks appeared to influence the performance of the overall population, few participants appeared non-susceptible to the manipulation (especially in Experiment 2 where the set-up did not allow for online adaptation of difficulty based on performance). Figure 1 displays the individual inverse efficiency scores from the population, showing that 9 participants (1 from Exp 1, 8 from Exp 2) showed comparable if not more proficient performance in the difficult condition. Because the goal of the study was to test for the effect of increased task demand on pain processing, the data from these 9 participants were excluded from subsequent analysis, because they did not establish higher demand for the more difficult versions of the tasks. We thus obtained a final sample of N = 25 in each experiment.

Violin plots and individual inverse efficiency data describing the difference between the two main conditions in (A) the N-Back (Exp. 1) and (B) Stroop task (Exp. 2). *** p < 0.001 for the effect of task difficulty. Inverse Efficiency scores refer to Response Times of correct responses (sec) penalized proportionally to the number of errors performed in the same condition. Red dots/lines refer to those specific participants for whom the difficult condition was associated with comparable/lower scores than the control condition. Int. = Stroop Interference. Contr. = Stroop Control.
Self-Pain
We then assessed whether sensitivity to nociceptive stimulation on one’s own body was influenced by the preceding task. Figure 2 and Table 1 report all data associated with self-related stimulations. In the analysis of explicit ratings, we found a significant main effect of Stimulation Intensity (3 levels) in both experiments, confirming that participants rated the three intensity levels as progressively more painful (Figure 2A-B). A similar main effect was observed also in the analysis of skin conductance response (Figure 2C-D) and heart rate variability (the latter only in Exp. 2). We also found that participants’ ratings and skin conductance response were influenced by the preceding task, in the shape of a Task Demand by Stimulation Intensity interaction. This effect, however, was observed only following the Stroop task (Exp. 2) but not following the N-Back (Exp. 1). We further explored this interaction through simpler models testing effects of Task for each stimulation intensity level. For both pain ratings and SCR, the interaction was explainable by a significant decreased response to HP following Stroop interference vs. control (t ≤ -2.14, p ≤ 0.044). In addition, there was a marginal increase in pain ratings for LP (t(22.56) = 1.80, p = 0.085), in line with what already observed in previous studies11,12 (Figure 3B). Finally, the analysis of confidence ratings was never associated to significant effects.

Self-Pain data. Pain intensity Stimulation and skin conductance response (SCR) results associated with (A,C) the N-Back task (Exp. 1), and (B,D) the Stroop task (Exp. 2). Red boxplots and data refer to nociceptive stimulations occurring after the difficult task condition (3-Back, Interference [Int.]), whereas blue boxplots/data refer to stimulations following the easy condition (0-Back, Control [Contr.]). Box plots are described in terms of median (horizontal middle line), interquartile range (box edges), and overall range of non-outlier data (whiskers). Dots refer to individual average values associated to each condition, and are considered outliers if exceeding 1.5 inter-quartile ranges from the median. **, *, ^ refer to significant task main effects for a given pain stimulation level, or to significant interactions between Task and pain intensity at p < 0.01, p<0.05, and 0.05<p<0.1 respectively. LP = Low Pain; MP = Medium Pain; HP = High Pain, Contr. = Stroop Control condition; Int. = Stroop Interference condition.

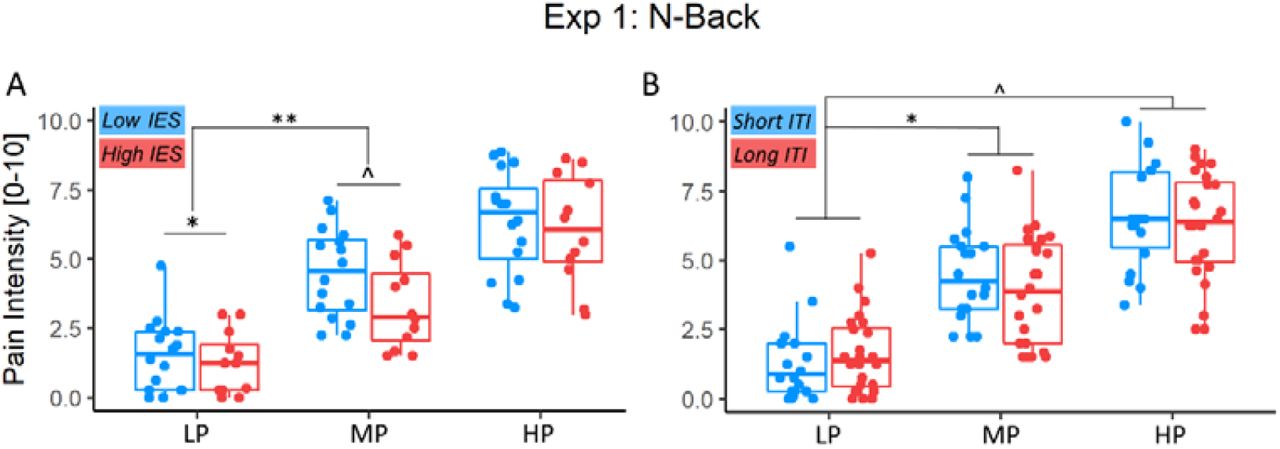
Performance effects on Self-Pain data. (A) Pain Intensity ratings associated with the N-Back task (Exp. 1), and (B) Heart Rate Variability associated with the Stroop task (Exp. 2). Red boxplots and data refer to nociceptive stimulations in half of the blocks with the highest IES (i.e., poorer performance), whereas blue boxplots/data refer the remaining blocks with the lowest IES (i.e., highest performance). “**”, “*”, “^” refer to simple IES effects for a given pain level, or significant interactions between IES and pain intensity at p < 0.01, p<0.05, and 0.05<p<0.1, respectively. Please note that, although data are divided into low vs. high IES categories for display purposes, the statistical analysis was carried out by modelling linearly raw IES values. IES = Inverse Efficiency Score; LP = Low Pain; MP = Medium Pain; HP = High Pain; HRV = Heart Rate Variability.
Self-Pain effects. We report the t-values associated with parameter estimates from linear mixed model analyses run on each experiment. Significant effect are highlighted based on the corresponding p-value (see legend). Conf. = confidence: R. = rating; SCR = skin conductance response; HRV = Heart Rate Variability; MP = Medium Pain; HP = High Pain
We also checked whether participants’ sensitivity to one’s pain changed as function of the performance of the preceding depleting task (3-Back and Stroop interference conditions). This was achieved by modelling participants’ inverse efficiency score (see Methods) from the previous block as a continuous between-subjects continuous predictor. Results are displayed in Table 2 and Figure 3, which reveal an interaction between Inverse Efficiency Score and Pain Stimulation Level for pain ratings (Exp. 1) and cardiac response (Exp. 2). Although in the main analysis, the Stroop Task only influenced the pain ratings and SCR, when taking into consideration participants’ performance we found an additional effect at the level of HRV, due to differential responses in HP (vs. LP) following tasks with poorer (vs. higher) performance (Figure 3B).
Self-Pain effects, analysis of Performance and Difficulty. We report the t-values associated with parameter estimates from linear mixed model analyses run on each experiment. Significant effect are highlighted based on the corresponding p-value. Conf. = confidence: R. = rating; MP = Medium Pain; HP = High Pain; IES = Inverse Efficiency Score; ITI = Inter-trial Interval; Cov. = Covariate of Interest (IES, ITI); SCR = skin conductance response; HRV = Heart Rate Variability.
Most critically, we also found that the performance of the 3-Back condition in Exp. 1 influenced pain ratings (Figure 3A), suggesting that blocks associated with poorer performance led to significant decreased sensitivity to MP (vs. LP) stimulations. A similar interaction was observed also at the level of HP (vs. LP), although only at a marginal level (t(134.45) = -1.76, p = 0.081). Finally, as in Exp. 1 difficulty was adjusted to stabilize performance across blocks (see Methods), it is possible that the effect observed could be confounded by differential difficulty. We therefore also modelled responses in Exp. 1 as function of the median inter-trial interval (ITI) from the preceding block. However, such parameter did not affect participants’ sensitivity to pain, neither as main effect nor in interaction with intensity (see Table 2).
Other-Pain
Next, we analysed pain ratings associated with videos of patients displaying painful/painless facial expressions. Figure 4 and Table 3 report all data associated with other-related stimulations. As expected, in the analysis of explicit ratings, we found a significant main effect of Pain Intensity in both experiments, confirming that participants rated the three intensity levels as progressively more painful (Figure 4A-B). Furthermore, we found that participants’ ratings were influenced by the preceding task, in the shape of a Task*Intensity interaction. This effect, however, was observed only following the Stroop task (Exp. 2) but not following the N-Back (Exp. 1). We further explored this interaction through simpler models testing effects of Task in each pain level, which was explained by a significant decreased response to HP following Stroop interference vs. control (t(67.11) = -2.97, p = 0.004; Figure 4B). Finally, the analysis of confidence ratings was never associated to significant effects.

Other-Pain data. Pain Intensity ratings results associated with (A) the N-Back task (Exp. 1), and (B) the Stroop task (Exp. 2). Red boxplots and data refer to videos presented after the difficult task condition (3-Back, Interference [Int.]), whereas cyan boxplots/data refer to videos following the easy condition (0-Back, Control [Contr.]). Box plots are described in terms of median (horizontal middle line), interquartile range (box edges), and overall range of non-outlier data (whiskers). Dots refer to individual average values associated to each condition, and are considered outliers if exceeding 1.5 inter-quartile ranges from the median. “**” refers to simple Task effect for HP, or significant interaction between Task and pain intensity at p<0.01. LP = Low Pain; MP = Medium Pain; HP = High Pain. Contr. = Stroop Control condition; Int. = Stroop Interference condition.
Other-Pain effects. We report the t-values associated with parameter estimates from linear mixed model analyses run on each experiment. Significant effect are highlighted based on the corresponding p-value. Conf. = confidence: R. = rating; MP = Medium Pain; HP = High Pain; SCR = skin conductance response; HRV = Heart Rate Variability.
We also checked whether participants’ sensitivity to other’s expressions changed as function of the performance of the preceding depleting task, through a similar procedure used for the analysis of Self-pain. Results are displayed in Table 4 and Figure 5. Overall, in the analysis of the Stroop task (Exp. 2) we found no effect of performance in any measure associated with the video-clips. Instead, and similarly to the case of Self-pain, participants’ performance influenced significantly the ratings of others’ MP (vs. LP) expressions, in the form of a IES*Intensity interaction (Figure 5A). Post-hoc analysis revealed that this interaction is explainable in terms of a positive effect of IES on the ratings of LP videos (t(75.78) = 2.40, p = 0.019), together with a marginal negative effect on the ratings of MPs videos (t(89.44) = -1.94, p = 0.055). Finally, the same interaction analysis was observed when modelling participants’ ratings in terms of task difficulty (3-Back task ITI) instead of performance (Figure 5B). Hence, at least for this analysis, we don’t know whether the effect should be interpretable in terms of performance, difficulty, or a combination of both. Overall, the analysis of the Other-Pain condition provided effects similar to those observed in the Self-Pain. However, these were limited to the case of explicit ratings, whereas no effect was associated with the analysis of the physiological responses.
Other-Pain effects, analysis of Performance and Difficulty. We report the t-values associated with parameter estimates from linear mixed model analyses run on each experiment. Significant effect are highlighted based on the corresponding p-value. Conf. = confidence: R. = rating; MP = Medium Pain; HP = High Pain; IES = Inverse Efficiency Score; ITI = Inter-trial Interval; Cov. = Covariate of Interest (IES, ITI); SCR = skin conductance response; HRV = Heart Rate Variability.

(A) Performance and (B) Difficulty effects on Other’s-Pain data from Exp. 1. Red boxplots and data refer to video-clips in half of the blocks with the highest IES (A) or longest ITI (B), whereas blue boxplots/data refer the remaining blocks with the lowest IES (A) or short (ITI). Please note that, although data are divided into low vs. high IES/ITI categories for display purposes, the statistical analysis is carried out by modelling linearly raw IES/ITI values. LP = Low Pain; MP = Medium Pain; HP = High Pain; IES = Inverse Efficiency Score; ITI = Inter-trial Interval.
Questionnaire Scores
We repeated the main analyses above by including the scores of relevant questionnaires of interest as covariates, in order to identify potential determinants of inter-individual differences in our effects. Specifically, we considered the Pain Catastrophizing Scale51, which is expected to tap key components involving attention and cognitive control of pain. As this questionnaire contains three subscales of interest (Rumination, Helplessness and Magnification), each of which could lead to plausible relevant effects, we report effects if associated with an α ≤ 0.0166 (corresponding to Bonferroni-corrected α ≤ 0.05 for three multiple tests). We found no effects associated in any of the three sub-scores in any of the measures of Self- and Other-Pain.
We also asked whether scores of the Interpersonal Reactivity Index52, a standardized questionnaire of individual empathic traits, may modulate the Other-Pain effects. As this questionnaire contains four subscales of interest (Personal Distress, Perspective Taking, Empathic Concern, Fantasy), we report effects if associated with an α ≤ 0.0125 (Bonferroni-corrected for four tests) for the Other-Pain condition. We found only a significant main effect of Personal Distress in the analysis of Pain intensity ratings, suggesting that individuals with higher scores are more prone to rate others’ expressions as more painful (Figure 6). This effect was found in Exp. 1, but not in Exp. 2 (Exp. 1: t29.04 = 3.20, p =0.003; Exp. 2: t23.02 = -0.26, p = 0.79; Figure 5). No other main/interaction effect was associated with any of the questionnaire scores.

Personal Distress effect on Other-Pain data. Individuals with higher scores on the Personal Distress subscale of IRI were more prone to rate others’ expressions as more painful after the N-Back task (A) but not after the Stroop task (B).
Discussion
We tested whether cognitive exertion influences the evaluation of subsequent one’s and other’s pain. For this purpose, we employed two cognitively demanding tasks, a working memory (Exp. 1: N-Back)44 and a cognitive control task (Exp. 2: Stroop)10,11,12, which both influenced the sensitivity to painful stimulations on one’s own body (consistent with previous research10), as measured by explicit ratings, galvanic skin response and heart rate variability. These effects were mirrored by a comparable decrease in subsequent assessment of facial expressions, with participants underrating those video-clips displaying the middle (Exp. 1: N-Back) or highest pain (Exp. 2: Stroop). This was observed either by comparing the effects of demanding condition to those associated with an easier control condition (Exp. 2: Stroop), or by modelling linearly the difficulty/performance of each demanding block (Exp. 1: N-Back). Finally, and specifically for the Stroop condition, we also found that cognitive control led to a mild hypersensitization towards self-directed low-pain stimulations (as previously suggested11,12). Overall, our results show that cognitive exertion alters the assessment others’ suffering, partly mirroring to what happens for first-hand pain experiences.
Stroop effects on Self-pain
The Stroop task influenced self-pain experience, by increasing sensitivity for LP stimuli, and decreasing it for HP ones. Although, to our knowledge, Stroop aftereffects on pain have never been tested as function of stimulation intensity, our findings may explain the heterogeneity in the literature, as previous research reported hyperalgesic effects of the Stroop for medium-low noxious stimulations (ratings corresponding to ∼4 on our scale)11,12, whereas others described hypoalgesia for more intense events (∼6)10. Traditionally, hyperalgesia following demanding tasks is interpreted in light of impaired top-down regulatory processes, which are elicited following nociceptive events to downplay aversive experiences, and promote coping reactions11,12. This interpretation fits well our findings with mild stimulations, but it does not account for what observed for intense nociceptive stimulations.
Our results reveal that cognitive exertion has a differential impact on mild and high pain stimulations, for which we suggest two possible interpretations. First, regulatory processes may be engaged in an active control of moderately (non life-threatening) painful situations to allow the pursuit of one’s everyday activity. Hence, for moderate levels of pain, increased attentional demands would impair efficient pain downregulation. Instead, when experiencing intense (or enduring) pain, the body may enter in a shock-like state in which suffering responses are automatically dulled65,66. Accordingly, the more a noxious stimulus is intense, the more pain regulation might shift from deliberate to automatic, thus leading to opposing depletion effects for high vs. low intensity. A second plausible interpretation would imply that cognitive exertion does not influence uniquely top-down regulatory processes, but interferes directly with the representation of pain. Indeed, recent accounts suggest that pain experience could be best interpreted within a Bayesian framework, where the brain estimates the (posterior) probability of potential body damage, based on the integration of sensory inputs and prior representations67–75. Within this framework, pain should be considered the result of an active inferential process which, under limited resources, could prove challenging for individuals, and lead poorer discrimination between low and high stimulations. This last interpretation would effectively fits all our findings.
In either case, our data provide a first clear evidence that cognitive control aftereffects on pain change as function of the intensity of the noxious stimulation, thus helping disambiguate an otherwise mixed literature.
N-Back effects on Self-pain
As for the effects of a memory task on self-pain, we found that participants’ performance in each 3-Back block was linearly coupled with the subsequent rating of medium/high pain stimulations: specifically, the poorer the performance (high IES) the higher the subsequent hypoalgesia (Figure 3A). Such effect could be interpreted as a result of cognitive depletion (as for the case of the Stroop), but only under the assumption that poor performance underlies a high level of cognitive fatigue already present during the task, and extending on the subsequent nociceptive stimulations.
An alternative interpretation spawns from motivational models of depletion and cognitive fatigue, according to which task subjective difficulty interacts with individual commitment in mobilizing effort76–78. Within this framework, a task perceived as too difficult would lead individuals to disengage, thus impacting only minimally the cognitive resources. Hence, participants with poor performance (high IES) should not necessarily have a high cognitive strain, but might have not committed to the task and, paradoxically, would have more resources available during the subsequent painful stimulation. We believe that this interpretation does not fit entirely our results. Indeed, while it is true that participants who disengaged from the task should be characterized by low proficiency (high IES), they should also be associated with low difficulty (short ITI). Indeed, as the task difficulty was continuously adapted to stabilize as much as possible performance across the population (see Methods), individuals who “gave up” should have rapidly converged towards the easiest task parameters. This was not observed in our study where, in the Self-Pain condition, the ITI did not influence participants’ sensitivity to pain. For this reason, participants’ high IES in our study most likely reflects proficiency fluctuations while they are actively engaged in the task.
Overall, although the results from the N-Back task are not entirely comparable with those from the Stroop, both sets of results converge in showing that task aftereffects impact the sensitivity to pain differentially as function of the noxious stimulation, with decreased sensitivity towards medium/high events.
Effects on Other-pain
The present study allowed us to compare opposing predictions between two accounts: the Broaden- and-Build theory predicted that cognitive exertion should influence self and other’s pain differentially, by increasing sensitivity for the former, at the expense of the latter; instead, Embodied accounts positing shared representation between self and others’ pain, suggest that cognitive exertion might affect judgments of others’ pain analogously to self-pain. Our results provide support to some predictions from both accounts. In line with the Broaden-and-Build theory, restrictions of one’s cognitive resources did decrease the sensitivity of medium/high painful expressions in both N-Back (as function of task performance and difficulty) and Stroop (relative to a neutral control condition). However, and most importantly, all the task-aftereffects observed in for other’s pain were observed also for the self-pain, with astonishing similarity in terms of the way in which the previous task was modelled (Task factor in Stroop, IES regressor in N-Back) and on the pain levels implicated (HP for Stroop, MP for N-Back). Hence, whatever the effects of each cognitive task on self-pain, similar effects were present also for the observation of others’ painful expression, thus providing strong support to the Embodied account.
Regardless of the winning model, our study sheds light on the role of mental fatigue in pain diagnosis, with relevant translational implications for healthcare practice. Physicians and nurses are often tasked with assessing patients’ pain under tiring working schedules. As such, they often underestimate patients’ pain1,4, a tendency present even during early university training79,80. Our data directly link underestimation of others’ pain to elevated attentional demands, such as keeping multiple information in working memory, and/or monitoring competing sources of information in order to prevent the selection of an incorrect response.
Limitations of the study and conclusive remarks
In our study, we excluded participants based on low pain sensitivity or non-susceptibility to the Stroop/N-Back. Although this criterion was established a priori, and data collection was conducted until a desired number of suitable participants was collected, two related limitations need to be underscored. The first is the sub-optimal nature of the task manipulation and pain intensity calibration, which might be vulnerable to factors like training, habituation, desensitization, etc. The second is the final sample, which might not be representative of the overall population, but only of those individuals most sensitive to pain and less proficient in the tasks employed.
Furthermore, differently from the case of the Stroop, N-Back aftereffects on pain sensitivity were found only when modelling individual IES as continuous predictor, but not in relation to the a priori designed control 0-Back. Ideally, the strongest effect would be associated with the most challenging condition which, in our case, refers to the 3-Back vs. 0-Back contrast in Experiment 1 (see Figure 1A). One possible explanation for this observation could be that memory tasks might be less suited than Stroop for inducing a depletion effect, as suggested by a recent meta-analysis81. Critically, cognitive control might be required also in the 0-Back control condition, where participants are asked to only respond to the presentation of a specific target letter (similarly to a “go/no-go” paradigm82), thus potentially questioning the effectiveness of this condition as a suitable control for cognitive control effects. Future studies will need to use a more suitable control (e.g. 1-Back) to test whether any discrepancy between working memory and inhibitory control in their relation to pain might hold.
Notwithstanding these limitations, our study demonstrates that the aftereffect of cognitive exertion on others’ pain judgment decreases the sensitivity towards the most intense stimulations, similarly to what observed in first-hand experiences. Healthcare personnel should be aware that high workload and strong cognitive fatigue might alter their diagnostic abilities.
Acknowledgments
We would like to thank Dr. Flavia Mancini and the team of Prof. Luis Garcia-Larrea (Dr. Maud Frot and Dr. Caroline Perchet) for all their assistance involving the nociceptive stimulations. We also thank Gwénaël Birot, Roberto Martuzzi, Leyla Loued-Khenissi and Loan Mattera for their support in data collection, Ben Meuleman and Lia Antico for their assistance in data analysis, and the Campus Biotech for the use of equipment and space. This work was supported by SNSF Grants n. PP00P1_183715 awarded to CCD, and n. 320030_182589 awarded to CCD and SS.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}