

Abstract
Background Current treatments for depression are limited by suboptimal efficacy, delayed response, and frequent side effects. Intermittent theta-burst stimulation (iTBS) is a non-invasive brain stimulation treatment which is FDA-approved for treatment-resistant depression. Recent studies suggest several improvements could be made to iTBS by 1) precision targeting of the left dorsolateral prefrontal cortex (L-DLPFC) to subgenual anterior cingulate cortex (sgACC) circuit, 2) treating with multiple sessions per day at spaced intervals and 3) applying a higher overall pulse dose of stimulation.
Objective Examine the feasibility, tolerability, and preliminary efficacy of an accelerated, high-dose, fcMRI-guided iTBS protocol for treatment-resistant depression (TRD) termed ‘Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT)’.
Methods Thirty-one participants with TRD received open-label SAINT. Resting-state functional connectivity MRI (fcMRI) was used to individually target the region of L-DLPFC most anti-correlated with sgACC. Fifty iTBS sessions (1800 pulses per session, 50-minute inter-session interval) were delivered as 10 daily sessions over 5 consecutive days at 90% resting motor threshold (adjusted for cortical depth). Neuropsychological testing was conducted before and after SAINT.
Results Twenty-eight of 31 participants (90.32%) met criteria for remission (≤10 on the MADRS) and all 31 were remitted on measures of suicidal ideation. Neuropsychological testing demonstrated no negative cognitive side-effects. There were no seizures or other severe adverse events.
Discussion Our highly accelerated, high-dose, iTBS protocol with fcMRI-guided targeting (SAINT) was well tolerated and safe. Efficacy was strikingly high, especially for this treatment-resistant population. Double-blinded sham-controlled trials are required to confirm the high remission rate found in this initial study.
Introduction
Depression is the leading cause of disability worldwide, and approximately 800,000 suicides are completed each year 1,2. Current FDA-approved antidepressant treatments do not achieve remission in the majority of patients with treatment-resistant depression (TRD) 3–5, are limited by tolerability 6 and have extended treatment durations, which do not match the imminent risk to suicidal patients 7–9. New antidepressant treatments are needed that are safe, tolerable, rapid-acting, durable, and more effective than current interventions.
Repetitive transcranial magnetic stimulation (rTMS) delivered to the left dorsolateral prefrontal cortex (L-DLPFC) is an FDA-approved non-invasive brain stimulation technique for TRD 10. rTMS involves passing an electrical current through a magnetic coil placed on the scalp, producing a high-intensity magnetic field that passes through the scalp, skull and meninges and excites neuronal tissue 11. Repeated high-frequency excitation of the same brain region results in successive strengthening of synapses through a process known as long-term potentiation (LTP) 12,13 causing lasting changes in functional connectivity 12,14. The antidepressant mechanism of rTMS is hypothesized to be the result of strengthened indirect inhibitory functional connectivity from L-DLPFC to sgACC 14,15.
A more efficient form of rTMS, known as intermittent theta-burst stimulation (iTBS), has been developed, which has significantly shortened the duration of treatment sessions from 37 minutes to 3 minutes 16 and produces equivalent antidepressant responses 17,18. FDA-approved rTMS and iTBS courses involve daily stimulation sessions for six weeks, achieving remission in 32% of patients and response in 49%, with an open-label, non-inferiority design 17. Studies suggest that the efficacy of iTBS could be improved by accelerated delivery 19–21, higher overall stimulation doses 9,22,23 and individualized targeting 14,24.
This study aimed to examine the feasibility, safety and preliminary efficacy of an accelerated, high-dose iTBS protocol using functional connectivity magnetic resonance imaging (fcMRI)-guided targeting. Five consecutive days of 10-daily iTBS sessions (1800 pulses per session) were delivered to the region of the L-DLPFC that was most anti-correlated to the sgACC in each individual 25. Individualized functional connectivity-guided targeting, accelerated delivery and high-dose stimulation were predicted to collectively result in higher response and remission rates than FDA-approved TMS protocols. This protocol was termed ‘Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT)’ to distinguish this protocol from other attempts at accelerated iTBS delivery without individualized targeting and/or high dose 26,27. We recently published a smaller series demonstrating efficacy in a cohort with extremely severe and treatment refractory depression 25.
Methods
Participants
Thirty-three participants with TRD (aged 19-78, 20 female) were recruited for this study. Twenty-four participants had a diagnosis of Major Depressive Disorder (MDD), six participants had a diagnosis of bipolar disorder (two bipolar 1) and three participants had depression in Parkinson’s Disease (DPD). Diagnoses of depression or bipolar disorder were confirmed by the study psychiatrist who performed the Mini International Neuropsychiatric Interview (MINI).
Participants were required to have a Hamilton Depression Rating Scale 17-item (HDRS-17) score higher than 20 and not have responded to at least one antidepressant medication (minimum trial duration of six weeks) to be eligible for the study. Urine samples were collected to screen for drug use and pregnancy. Participants were recruited through the Depression Research Clinic at Stanford University, Facebook advertising and clinic referrals. All participants provided written informed consent and the study was approved by the Stanford University Institutional Review Board.
One participant was excluded for having a motor threshold that was too high (>90% machine output) and one participant with a history of high anxiety dropped out after the first day of stimulation due to high anxiety levels (Young Mania Rating Scale (YMRS) and HDRS-17 scores had not increased from baseline). This resulted in a final participant sample of 31 participants (aged 19-78, 19 female). See Table 1 for participant demographic information and treatment history. Participants were required to maintain the same antidepressant regimen throughout the study enrollment (see Supplementary Table 7 for information regarding the medication participants were taking during study enrollment).
Demographic information and treatment history for all participants (n=31)
Functional magnetic resonance imaging (fMRI)
Before the stimulation course, each participant had both structural magnetic resonance imaging (MRI) and resting-state functional MRI (fMRI) scans. All participants were screened for MRI safety prior to any scanning procedures. All MRI scans were acquired using a 3T GE Discovery MR750 scanner with a 32-channel imaging coil at the Center for Cognitive and Neurobiological Imaging at Stanford, using a 3x accelerated multiband imaging sequence (TR=2 seconds). The resting state scan consisted of a single 8-minute eyes-open resting scan.
Two participants did not take part in the MRI portion of the study as one participant had a BMI which was above the limit of the scanner (BMI >35) and one participant had a spinal stimulator. For these participants, their heads were registered to the MNI brain and anatomical coordinates previously shown to result in superior clinical outcomes compared to the standard 5cm rule were used for coil placement (−46, 45, 38) 82. This target has also shown to be more anti-correlated to the sgACC than the area identified by the 5cm rule 14.
Stanford Accelerated Intelligent Neuromodulation Therapy
A Magventure Magpro X100 (MagVenture A/S, Denmark) system was used to deliver sessions of iTBS; 60 cycles of 10 bursts of 3 pulses at 50Hz were delivered in 2 second trains (5Hz) with an 8 second inter-train interval. Stimulation sessions were delivered hourly 19–21. Ten sessions were applied per day (18,000 pulses/day) for five consecutive days (90,000 pulses in total). See Figure 2. Stimulation was delivered at 90% resting motor threshold 83,84. A depth correction 85 was applied to the resting motor threshold to adjust for difference in the cortical depth of the individual’s functional target compared to the primary motor cortex in order to consistently achieve 90% rMT in the intended functional target but stimulation was never delivered above 120% rMT for safety. The Localite Neuronavigation System (Localite GmbH, Sankt Augustin, Germany) was used to position the TMS coil over the individualized stimulation target. Participants in full remission prior to the end of the five-day stimulation course, were given the option to either finish early or complete the full course. One participant with a diagnosis of Bipolar type 1 finished treatment after the first day and one participant with Parkinson’s finished treatment after 3 days. All other participants completed the full five-day treatment course.
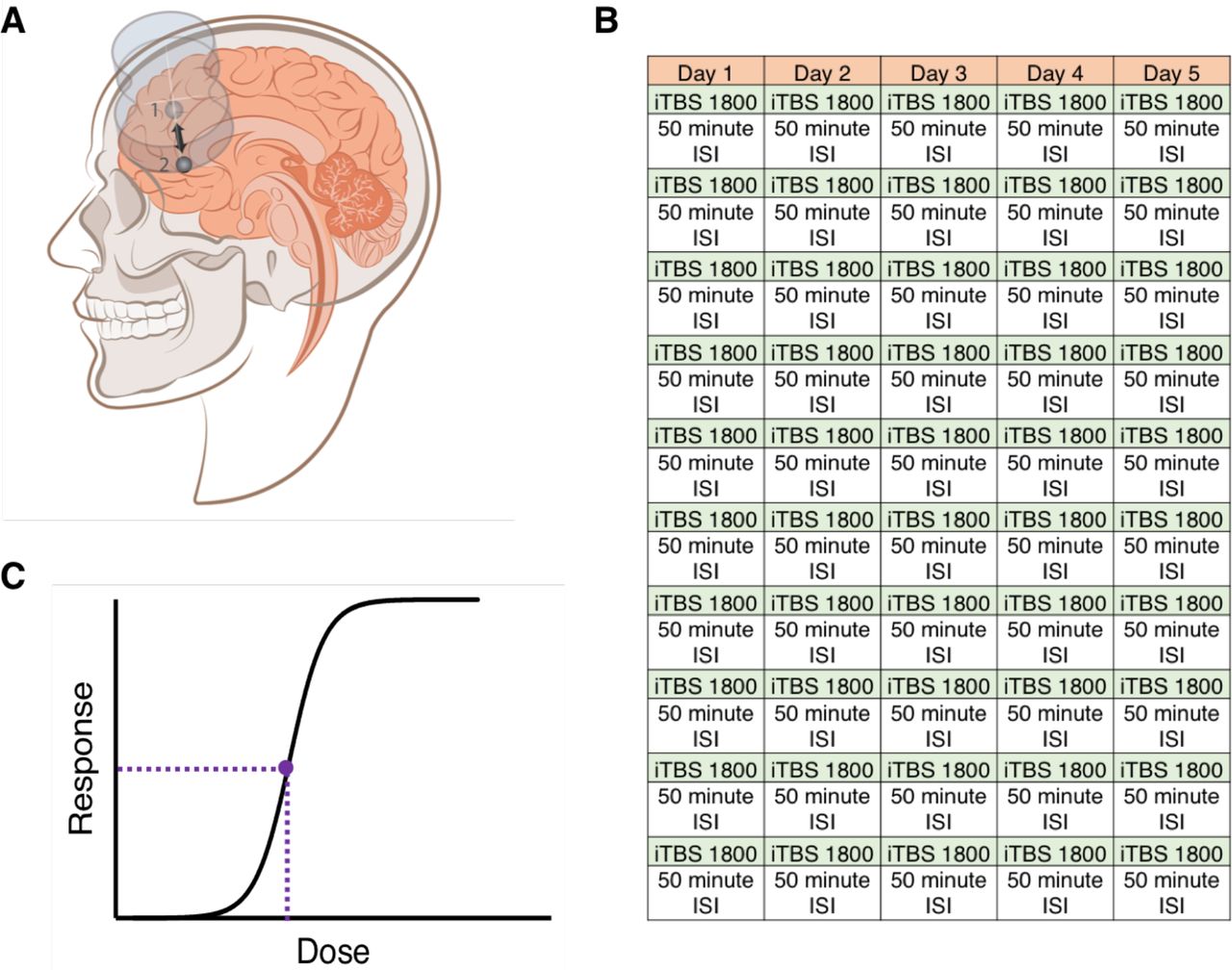
This figure illustrates the three factors which make SAINT different from current FDA-approved iTBS protocols: Precise targeting (A), accelerated delivery (B) and high pulse dose [both per session (B) and overall (C)]. A) Stimulation was delivered to the region of the L-DLPFC (1) which was most anti-correlated to the sgACC (2) due to previous neuroimaging findings which suggest the higher the anti-correlation between the stimulated region of the L-DLPFC and the sgACC, the better the clinical outcome 14,24,44. B) Unlike, FDA-approved protocols which only deliver one iTBS session per day, our SAINT protocol delivered 10 sessions per day. iTBS sessions were delivered 50 minutes apart because previous research has shown that iTBS sessions delivered 50-90 minutes apart have a cumulative effect 19–21. In comparison, iTBS sessions delivered only 40 minutes apart or less, have shown not have a cumulative effect 19–21,40,42. 1800 pulses per session was chosen as this is the only pulse dose that has been explored in a blinded iTBS trial 49. Additionally, 1800 pulses has been shown to produce long-lasting changes in cortical excitability 100 and optimally produce intended cellular changes 101. C) Our study administered the highest overall pulse-dose of any published study to date. A dose-response curve has never been constructed for clinical TMS but a previous study showed 61% of non-responders to a standard 6-week TMS course responded with further treatment 23 suggesting that FDA-approved protocols are under-dosing (the purple dotted line provides an example of where the FDA-approved dose could be on the curve). Our SAINT protocol delivered 5x the FDA-approved dose. See supplementary material for more information regarding protocol development.
Clinical assessments
Prior to receiving any stimulation, participants’ depressive symptoms and suicidal ideation were assessed using the Hamilton Depression Rating Scale-17 item (HDRS-17), Montgomery-Asberg Depression Rating Scale (MADRS) and Columbia-Suicide Severity Rating Scale (C-SSRS, suicidal ideation subscale). A self-report measure was also used; the Beck Depression Inventory II (BDI-II). The degree of treatment-resistance was calculated using the Maudsley Staging Method 86, and symptoms of mania were screened for using the Young Mania Rating Scale (YMRS). At the end of each day of stimulation (ten sessions), depressive symptoms were assessed using the Hamilton Depression Rating Scale 6-item (HDRS-6); participants also completed the BDI-II. The YMRS was completed daily to ensure hypomania had not been induced in any participants 87–89. The same clinical assessments used at baseline were conducted approximately 72 hours after the stimulation course (immediate follow-up) as well as two weeks and one month after the stimulation course in order to assess the durability of the response.
A neuropsychological test battery was administered before SAINT and approximately 72 hours after the SAINT course in order to capture any neurocognitive side effects. The Hopkins Verbal Learning Test – Revised (HVLT-R) 90, the Brief Visuospatial Memory Test – Revised (BVMT-R) 91, subtests from the Wechsler Adult Intelligence Scale (4th Ed.; WAIS-IV) 92 and various tests from the Delis Kaplan Executive Function System (D-KEFS) 93 were used. These neuropsychological tests have been shown to have good psychometric properties 90,91,93,94 and assessed verbal learning and memory, visuospatial learning and memory, working memory, attention, cognitive inhibition, cognitive switching, problem solving, and verbal fluency. See supplementary material for detailed information about the neuropsychological test battery.
fMRI analysis for target generation
Personalized L-DLPFC targets were generated for each participant using the resting-state scan. All analyses were conducted in a participant’s own brain space (i.e., not warped to standardized-brain space). Resting-state scans were pre-processed according to typical methods using Statistical Parametric Mapping (SPM12) software. The resting-state scans were motion corrected and resliced. The T1 weighted structural scan was then co-registered with the resting-state scans. The resting-state scans were then spatially smoothed with a 3mm Gaussian kernel, detrended using a linear model of the global signal 95, and band-pass filtered to preserve the typical resting-state frequencies (0.1Hz-0.01Hz). Next, the estimation parameters to warp the T1 weighted structural image into Montreal Neurological Institute (MNI) space was calculated using SPM segmentations based on tissue probability maps. These normalization parameters were inverted and applied to MNI space regions of interests (ROIs) for the L-DLPFC (Brodmann area 46) and the sgACC (BA25). This inverse normalization served to map the MNI space ROIs onto the individual participant’s brain. The participant-space ROIs were then resliced, smoothed, and binarized to match the dimensions of the resting state scans.
The participant-space ROI for the L-DLPFC formed the search area for the optimal TMS coil placement. Two separate algorithms were used to determine coil placement. The first algorithm sorted each of the DLPFC and sgACC voxels into functional sub-units using a hierarchical agglomerative clustering algorithm. Median time series were then created for each functional subunit and the correlation coefficients were calculated between all median time series extracted from all functional subunits of the L-DLPFC and sgACC. The second algorithm determined the optimal L-DLPFC subunit to target based on three factors: the net correlation/anti-correlation of the L-DLPFC subunit with sgACC subunits, the size of the subunit and the spatial concentration of the subunit. See supplementary methods for more details on these algorithms. 3D maps of the whole brain correlation coefficient of the selected L-DLPFC subunit were then created and used to target the coil placement using the Localite TMS Navigation software (Localite GmbH, Sankt Augustin, Germany).
Clinical outcome analysis
All statistical analyses were conducted using IBM SPSS Version 22. The level of statistical significance was set at p = 0.05. Missing data were not imputed for any statistical analysis. Statistical analyses were planned independently by BSB and reviewed by EJC, NWR, BJ and AFS. These analyses were then carried out by BSB and EJC.
Our primary outcome measure was change in MADRS scores from baseline to immediately following SAINT, and MADRS scores were used to calculate response and remission rates. Reductions in HDRS-17, HDRS-6 and BDI-II scores were used as secondary outcome measures of depression severity. Response was defined as ≥50% reduction in these scales. Remission was defined as MADRS score ≤10 96, ≤7 on HDRS-17 97 ≤4 on the HDRS-6 98, BDI≤12 99. A floor effect of SAINT treatment was observed across all scales, and initial linear mixed models produced residuals that were not normally distributed. Thus, changes in MADRS, HDRS-17, and BDI-II were assessed with generalized linear mixed models (GLMM) that used a compound symmetry covariance structure, Satterthwaite approximation of degrees of freedom, and robust estimation of coefficients to handle violations of model assumptions. Fixed effects of time, diagnosis (MDD vs. non-MDD), and prior non-response to conventional rTMS were assessed, as well as time × diagnosis and time × response interactions. All post-hoc pairwise comparisons were Bonferroni-corrected.
Eleven participants were re-treated once their symptoms returned to baseline and again met study entry criteria. A similar GLMM was used to assess whether SAINT re-treatment was able to produce equivalent antidepressant responses. Fixed effects of time, treatment course, and their interaction were assessed.
Daily HDRS-6 scores were used to calculate the number of days of stimulation required to reach responder criterion (<50% HDRS-6) and remission criterion (<5 on HDRS-6). Kaplan-Meier survival analysis using the Breslow test of equality of survival distributions was used to determine if there were significant differences in the number of days to reach response and remission criteria for participants who had a history of conventional rTMS non-response compared to those who did not.
Suicidality was assessed using the Columbia Suicide Severity Rating Scale (C-SSRS, suicidal ideation subscale), item 3 of the HDRS-17, and item 10 of the MADRS. Response was defined as ≥50% reduction in these scores from baseline and remission was defined as a score of 0. Response was only calculated if the baseline score was >0. Remission was defined as a score of 0 for each of these scales. Scores were ordinal and changes in scores were assessed with generalized linear models with a multinomial link, compound symmetry covariance structure, Satterthwaite approximation of degrees of freedom, and robust estimation of coefficients to handle violations of model assumptions.
Scores on the neuropsychological tests before and after SAINT were compared using paired t-tests. The data for the Hopkins Verbal Learning Test (HVLT) total score, HVLT Delayed Recall score, the Brief Visuospatial Memory Test (BVMT)-Delayed Recall and the number of rule violations on the D-KEFS Tower Test violated the assumption of normality so non-parametric (Wilcoxon signed-rank) tests were used to evaluate SAINT-induced changes in performance on these three tasks. Neuropsychological test data were available for 22 participants.
Results
Safety
No serious adverse events occurred. The only side-effects participants reported were fatigue and some discomfort at both the stimulation site and in the facial muscles during stimulation. The neuropsychological test battery showed no negative cognitive side-effects following SAINT. Performance significantly improved on measures of cognitive inhibition [D-KEFS color-word inhibition task; t(20)=2.98, p=.007, d=.65], cognitive switching [DKEFS trail making test condition 4, Alternating Letter-Number Switching; t(19)=2.50, p=.02, d=.56], problem solving [DKEFS Tower Test Total Achievement Score; t(20)=−2.70, p=.01, d=.59]; and rule violations on the D-KEFS Tower Test; z=−2.68, p=.007, r=.4]. Due to the large number of comparisons made, the significant improvements in performance observed did not survive the correction for multiple comparisons (Bonferroni-corrected significance level p<.004). There were no significant changes on any of the other neurocognitive tasks, see supplementary material.
Depression symptoms
Depressive symptoms decreased from baseline immediately following SAINT with an 87.66% reduction in the mean Montgomery-Asberg Depression Rating Scale (MADRS) score from 37.68 (SD=7.24) to 4.65 (SD=6.46). Generalized linear mixed-model (GLMM) analysis revealed a significant effect of time (F3,27=106.742, P<.001) on mean MADRS scores with all follow-up time points being significantly lower than baseline (Bonferroni-corrected pairwise comparisons, P<.001). These results were recapitulated for the Hamilton Depression Rating Scale (HDRS-17, F3,26=124.128, P<.001) and the Beck Depression Inventory (BDI, F3,29=33.692, P<.001). The response rate (≥50% reduction in MADRS) was 90.32%, and all responders were in remission (MADRS score ≤10). Results were similar across all clinical assessments (see Table 2). One month following SAINT, 59% of participants continued to meet responder criteria (see Supplementary Table 1 for response rates at one month).
A major hypothesis of SAINT is that conventional rTMS delivers insufficient cumulative stimulation to induce response and remission from depression for some patients. We tested this by including participants who had a history of non-response to conventional rTMS (rTMS non-responders, n=13). We found that conventional rTMS non-responders had significantly greater MADRS scores (GLMM, responder, F1,14=15.875, P=.001; responder × time, F3,35=3.837, P=.018) at all time points except baseline (Bonferroni-corrected pairwise comparisons, P<.001) compared to the rest of the participant sample (see Figure 2 and Supplementary Tables 5 and 6).
Clinical assessment scores for all participants immediately following SAINT; mean (SD, n) or % (n)
Days of treatment until response and remission
The mean number of days of SAINT until participants met the response criterion (≥50% reduction in HDRS-6 score) was 2.46 (SD=1.26, ~25 10-min treatments, n=28, daily HDRS-6 scores missing for 2 participants, 1 participant did not respond by the HDRS-6 criterion), and the mean number of days to achieve remission (HDRS-6 score <5) was 2.96 (SD=1.48, ~30 10-min treatments, n=26, 3 participants did not achieve remission by the HDRS-6 criterion). Similar time courses were seen for participants with MDD. See Figure 3 for percentage change in HDRS-6 score with each day of stimulation, for all participants (2A) and participants with MDD (2B).
Kaplan-Meier survival analysis revealed that participants who had previously not responded to a 6-week rTMS treatment course (n=13) required more days of treatment to achieve responder criterion [X2=8.047, P=.005, mean 3.08 days (SD=0.67), ~31 treatments] and remission criterion [X2=7.894, P=.005, mean 3.70 days, (SD=.95), ~37 treatments). See Figure 4. None of the rTMS non-responders met responder criterion after the first day of aiTBS; notably, the first day of SAINT provides an equivalent amount of stimulation as six weeks of FDA-approved iTBS.

Percentage change in MADRS score immediately following the five-day stimulation course, two weeks and four weeks afterwards for TMS non-responders (red, n=13) and all other participants (blue, n=18). rTMS non-responses showed significantly lower percentage reduction in MADRS score at all timepoints after SAINT than the rest of the participant sample: (Immediate, n=18/13, p<0.05; 2 weeks, n=18/13 p<0.01; 4 weeks, n=17/12 p<0.01)

Mean percentage change in Hamilton Depression Rating Scale score (6-item version) with each day of stimulation for A) All participants (n=29, daily HDRS-6 scores missing for two participants), B) MDD participants (n=21, daily HDRS-6 scores missing for one participant). Dotted lines indicate responder criteria and error bars represent standard error.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean percentage change in Hamilton Depression Rating Scale score (6-item version) with each day of stimulation for A) All TMS non-responders (n=13), B) All other participants (n=16), C) MDD TMS non-responders (n= 10), D) All other MDD participants (n=11). Dotted lines indicate responder criteria and error bars represent standard error.
Re-treatment efficacy
Eleven participants were re-treated after they no longer met responder criterion and again met study entry criteria (mean time between treatments was 20.27 weeks, SD=14.07). There were no significant differences in MADRS scores between treatment courses (GLMM, F1,155=0.192, P=0.662), nor was there a treatment × time interaction (GLMM, F3,155=0.607, P=0.611). Baseline and follow up MADRS scores were all similar between treatment courses (Bonferroni-corrected pairwise comparisons, P>0.05). See Table 3 for percentage change in MADRS score for initial SAINT and re-treatment for each participant.
Percentage change in MADRS score for initial and re-treatment
Suicidality scales
Changes in suicidality scales were assessed with generalized linear modeling (GLM) with a multinomial link. Following SAINT there were significant reductions in the Columbia-Suicide Severity Rating Scale [(C-SSRS, suicidal ideation subscale) (GLM, X2(2)=17.086, P<0.001)], item 3 of the HDRS-17 (GLM, X2(3)=48.976, P<0.001), and item 10 of the MADRS (GLM, X2(3)=59.133, P<0.001) at all follow up time points (X2, P<0.001). All participants remitted on these measures of suicidal ideation (see Table 2). One month following SAINT, 95% of participants continued to be remitted (see Supplementary Tables 3 and 4).
Discussion
The aim of this study was to examine the safety, feasibility and preliminary efficacy of an accelerated high-dose iTBS, fcMRI-guided treatment protocol (SAINT) for treatment-resistant depression (TRD). We found that SAINT significantly reduced depressive symptoms and suicidal ideation in patients with severe TRD within 5 days without negative cognitive side-effects or other adverse events. The 90% remission rate we observed is substantially higher than remission rates for open-label studies using standard FDA-approved rTMS treatment protocols 17,31,32. This is also higher than what has been reported for electroconvulsive therapy (ECT) treatment of TRD (~48%4) and for ketamine treatment of TRD (14.3-66.6%33–35). This remission rate was observed despite the inclusion of participants who had previously failed FDA-approved rTMS and/or ECT treatments. The potential high efficacy of SAINT may be due to the combination of the accelerated delivery of iTBS sessions, the high-dose of stimulation and the individualized targeting method used.
Although our initial observed response and remission rates are atypically high compared to other studies that have tested rTMS protocols for treatment of depression (rTMS/iTBS/cTBS), similar response rates have been found in deep brain stimulation trials for depression and Parkinson’s Disease 36,37. The high efficacy of our SAINT protocol complements evidence from basic neuroscience research and human physiology data, which suggest that multiple spaced daily iTBS sessions have an enhanced effect compared to the same number of single daily sessions 19–21,38,39. Studies that have applied theta-burst protocols (cTBS/iTBS) to the motor cortex in humans have shown that two spaced stimulation sessions produce greater 40 and longer lasting 39,41 changes in cortical excitability than single stimulation sessions. Rodent studies conducted using hippocampal slices have shown that multiple iTBS sessions delivered with inter-session intervals of 50-90 minutes have a cumulative effect on dendritic spine enlargement, a process involved in synaptic strengthening 19–21,38. In comparison, iTBS sessions delivered with inter-session intervals of 40 minutes or less do not have a cumulative effect on dendritic spines19–21. Similarly, two iTBS sessions delivered to the prefrontal or motor cortex in humans only 15 minutes apart have shown not to increase cortical excitability more than a single iTBS session 40,42. This could explain the limited efficacy of a previously reported accelerated iTBS protocol, which used an inter-session interval of only 15 minutes 26,27.
The individualized targeting method used in our study may have also contributed to the high response and remission rates. The L-DLPFC is a large brain area that consists of several subregions, some of which are correlated and some anti-correlated with sgACC activity 43. Targeting rTMS to the subregions of L-DLPFC that have higher functional anti-correlation with sgACC have been shown to produce a superior antidepressant response 14,24,44. Defining L-DLPFC using common techniques such as scalp-based measurements, structural MRI scans or fMRI activation patterns could result in stimulating a subregion of the L-DLPFC that is correlated rather than anti-correlated with the sgACC and therefore not drive the desired increase in anti-correlation between L-DLPFC and the sgACC 45. The standard ‘5cm rule’ scalp-based measurement has been shown to miss the L-DLPFC completely in >1/3 of cases 46. A retrospective study conducted by Fox and colleagues found that individual differences in the degree of anti-correlation between the stimulated subregion of the L-DLPFC and the sgACC accounted for over 70% of the variability in clinical efficacy 14. A recent interleaved TMS-fMRI study showed that stimulating the subregion of the L-DLPFC that displays the greatest degree of functional connectivity with the sgACC resulted in stimulation propagation to the sgACC in all participants 47. In comparison, in a separate study when the L-DLPFC was defined anatomically (border of BA9/BA46), stimulation propagated to the sgACC in only 44% of participants 48. In the aiTBS study by the Baeken group 27 and a blinded iTBS trial 49 the same anatomical target (border of BA9/BA46) was utilized, which may have contributed to the limited efficacy of these approaches. By stimulating the subregion of the L-DLPFC that is most anti-correlated with the sgACC in each individual in this study, we may have reduced this variability in signal propagation and maximized treatment efficacy.
The high efficacy of our SAINT protocol also suggests that FDA-approved protocols may be under-dosing. Our protocol administered five-times the pulse dose of the FDA-approved iTBS protocol (90,000 pulses in comparison to the standard 18,000 iTBS pulses17). Prior studies found that 61% of individuals who do not respond to an initial six weeks of stimulation responded with additional rTMS treatment sessions 23, and higher pulse doses are associated with higher response and remission rates 50,51. Our SAINT protocol applied the equivalent amount of stimulation as a six-week treatment protocol each day of stimulation (18,000 pulses/day 17). Thirty-one percent of participants in our study met responder criteria after the first day of stimulation (n=9/29, daily HDRS-6 missing for 2 participants), this response rate is equivalent to response rates found after six-weeks of daily iTBS/rTMS sessions in individuals of this treatment-resistance level 29,30,52,53. None of the prior rTMS non-responders in our study responded after the first day of SAINT (see Figure 4). These data indicate that a non-response to a standard six-week treatment protocol may reflect the need for a higher stimulation dose, for the majority of patients 23, which matches with recent trajectory data 54. The apparent need for a higher number of stimulation pulses is consistent with other neuromodulation modalities, such as deep brain stimulation in Parkinson’s where a mean of 500,000 pulses of stimulation are delivered to the subthalamic nucleus (STN) or the globus pallidus (GPi) each day 55. The need for a higher overall dose of stimulation may have also contributed to the limited efficacy of a previous attempt of an accelerated iTBS protocol, which only delivered 32,400 pulses 26. Our study administered the highest number of pulses per day and highest overall pulse-dose of any study we are currently aware of 25.
Prior rTMS non-responders in our study not only required more stimulation sessions to induce a clinically significant response but also showed less-durable responses than the rest of the participant sample. The high relapse rate at one month in this subsample is reflective of the ECT data which show general relapse rates of 62.7% at 3 months and 78% at 6 months 56 with 25% of treatment-resistant individuals relapsing after one week 57 and an average length of wellness of 8.6 weeks 58. It is possible that depressed individuals with a higher degree of treatment-resistance display neuroplasticity impairments 59. The higher number of stimulation sessions required to induce antidepressant responses could be due to deficits in processes involved in the early stages of LTP, such as AMPA receptor phosphorylation 59,60. The shorter duration of antidepressant responses could be the result of dysfunction in later LTP processes that mediate long-lasting changes to synaptic strength 41. These processes include the synthesis of new proteins and gene expression changes such as the activation of transcription factors (e.g. CREB) and the induction of plasticity-enhancing genes such as BDNF 59. Highly treatment-resistant individuals may require maintenance iTBS therapy 61 or even implanted epidural cortical stimulators 62,63 to sustain antidepressant responses.
The short duration of our SAINT protocol, the apparent reproducibility of responses and the lack of cognitive side-effects, provide potential benefits over currently available treatments. The short duration of our SAINT protocol means SAINT could provide a rapid means of treating patients with active suicidality. Ketamine and ECT are currently available alternatives. Ketamine/s-ketamine has recently been FDA-approved for treatment-resistant depression; however, ketamine has several limitations. Approximately 11% of patients report the dissociative symptoms as very disturbing 64, remission rates for ketamine/s-ketamine are lower than the remission rate we observed for SAINT 33,35,65, very few studies have investigated the anti-depressant efficacy of ketamine beyond a single infusion 66,67 and the opioid mechanism of action poses a potential risk 68. The other available rapid-acting treatment is ECT, for which less than 2% of eligible patients receive due to concerns regarding cognitive side-effects and stigma 69,70. In the majority of patients, ECT also takes two weeks or longer to produce remission from suicidal ideation 71.
Our study has several limitations. It is limited by the small sample size and open-label design; a double-blind controlled trial is required to determine the efficacy of our SAINT protocol in comparison to an identical schedule of sham stimulation sessions. However, individuals with the same degree of treatment-refractoriness as the participants included in this study (severe treatment-resistance; >11 Maudsley Staging Method), have previously shown no placebo response to iTBS sessions of 1800 pulses 49. Additionally, the most recent deep brain stimulation (DBS) sgACC trial for TRD included individuals with similar treatment-resistance levels to the patients in this report and had a response rate of only 20% 72. A greater degree of placebo response would be expected for DBS as placebo response has generally been related to the degree of invasiveness of the intervention 73. Other limitations of our study include the single stimulation site 74–76, the use of fixed stimulation frequencies 54,77, fixed inter-session intervals 77,78 and the lack of state-dependent stimulation 79. It is possible that different stimulation sites may be optimal for certain patients based on their symptom profile 74–76. The use of individualized stimulation frequencies may result in quicker and more durable responses 77,80. Some individuals may require slightly different inter-session intervals due to differences in cortical excitability profiles 78,81. Finally, recent studies have shown that applying stimulation in particular brain states using real-time electroencephalography (EEG)-triggered transcranial magnetic stimulation (EEG-TMS) can increase cortical responses to stimulation 79. Limitations regarding the clinical application of SAINT include the high cost and additional time required to use neuronavigation equipment, acquire MRI scans and process the resulting data.
In conclusion, the high-dose of stimulation, accelerated delivery and fcMRI-guided individualized targeting method are preliminarily safe, well tolerated, feasible, and associated with high rates of remission from depressive episodes. The high remission rate we observed with SAINT was found despite the inclusion of participants who had previously not responded to rTMS and/or ECT. These rates are almost double those observed in TRD individuals receiving open-label ECT 4, which is currently the ‘gold standard’ treatment for TRD. Our data suggest that FDA-approved TMS protocols may be under-dosing and could potentially benefit from individualized targeting methods and accelerated delivery. The efficacy of SAINT in treating suicidal ideation and the short duration of the protocol suggest SAINT could provide a means of rapidly ensuring the safety of suicidal patients. Larger, double-blinded, placebo-controlled trials are required to confirm the promisingly high response and remission rates found in this initial study.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.




