

ABSTRACT
Background Clinical evidence suggests that Parkinson’s Disease (PD) patients are risk-averse, but clear experimental evidence of this is surprisingly lacking. Anti-parkinsonian therapy has been reported to increase tolerance for risk, though findings have been mixed, and it has remained unclear whether this results from altered attitudes towards potential rewards, potential punishments or both. In some cases, alterations in reinforcement learning may have also been responsible for the findings.
Objective To disambiguate the effects of PD and its therapy on attitudes towards rewards vs. losses in the context of risky decision making unconfounded by reinforcement learning.
Method 36 patients with idiopathic PD receiving levodopa monotherapy and 36 healthy age-matched controls performed two behavioural economic tasks aimed at quantifying 1) risk tolerance/ aversion in the gain frame and 2) valuation of gains relative to losses. PD patients performed the tasks on and off their usual dose of levodopa in randomized order; the healthy controls performed the same tasks twice.
Results Relative to the healthy controls, unmedicated PD patients showed significant risk aversion in the gain frame, which was normalized by levodopa. There was no difference between PD patients and controls in valuation of gains relative to losses. In addition, across both tasks and regardless of medication state, choices of the PD patients were more driven by expected values of the prospects than were the choices made by controls.
Conclusion Dopamine deficiency in PD was associated with risk aversion but not with an altered valuation of gains relative to losses.
Financial disclosure/conflict of interest: This work was supported by operating grant MOP-130566 from the Canadian Institutes of Health Research. JB was supported by Canada Research Chair 950-228984 and the Marianne Koerner Chair in Brain Diseases. AJS is supported by the Canada Research Chairs program. Authors declare no competing interests.
INTRODUCTION
Clinical evidence suggests that drug-naïve Parkinson’s disease (PD) patients are rigid and risk-averse (1,2), although experimental evidence of this is sparse. On the other hand, dopaminergic therapy, particularly direct dopamine agonists, can cause impulse control disorders with compulsive risky reward seeking such as pathological gambling (3).
The mechanisms behind this are not entirely clear. Though many studies have examined decision making under uncertainty and risk in PD, most have used tasks requiring more than a single cognitive operation, such as the Iowa Gambling Task, which confounds maladaptive risky choice with reinforcement learning. Thus, although a recent meta-analysis concluded that PD patients were impaired on the Iowa Gambling Task independent of medication (4), this could stem from either maladaptive decision making or well-documented reinforcement learning deficits (5)(6).
Work using other well-established neuropsychological decision-making tasks, such as the Cambridge Gambling Task, Game of Dice, and Balloon Analogue Risk Task have yielded mixed findings. Some reported that medicated PD patients showed increased risk taking compared to unmedicated patients or healthy controls (7)(8)(9), but others did not find this (10)(11)(12). Studies with the Cambridge Gambling Task have mainly suggested medication-driven impulsivity of choice in the patients (13) (14).
Studies using behavioural economic tasks, which permit isolation and mechanistic analysis of cognitive primitives involved in choice under risk, have also produced mixed findings. While three studies found that dopaminergic therapy made patients more risk tolerant in the context of gain only (15) and mixed gambles (16)(17), two studies did not find this (18) (19). Regarding the mechanisms, two studies suggested that medication promoted riskier choice by amplifying the subjective value of rewards (15)(16), and one suggested it did so in a value-independent manner (17). Loss aversion, a tendency to avoid losses more than to seek equivalent size gains, has been hypothesized in PD based on dopamine’s role in the relative valuation of rewards and punishments (20). However, studies have not produced clear evidence of loss aversion in PD, instead suggesting complex effects, possibly modulated by a history of depression (17)(18). Only one study has clearly shown that PD patients were risk-averse in the OFF state relative to controls (16), but only a partial OFF state was achieved, in which levodopa but not dopamine agonists or other antiparkinsonian medications were withdrawn. Given the mixed gamble design in that study, it also unclear whether the risk aversion was driven by underweighting of gains or overweighting of losses. Overall, there appears to be some evidence that dopaminergic therapy produces riskier choice in the context of mixed gambles, but it has remained unclear whether this is because of altered attitudes towards potential rewards, potential punishments or both.
To resolve this issue and disambiguate the effects of PD and its therapy on attitudes towards rewards vs. losses in the context of risky decision making, we tested PD patients treated with levodopa monotherapy in ON and OFF states, as well as matched controls, using two behavioural economic tasks. A two-choice lottery Vancouver Gambling Task (21)(19) was used to assess willingness to take risks in the gain frame (i.e. choose larger less likely rewards) without the possibility of loss or influence of loss aversion. To measure weighing of gains relative to losses, we used the Vancouver Roulette Task featuring mixed gambles with varying bet sizes. Both tasks permitted to estimate the influence of prospect characteristics (probabilities, magnitudes and expected values) on choice. Neither required reinforcement learning.
We hypothesized that relative to matched healthy controls, patients in the OFF state would demonstrate risk aversion in the gain frame and an unwillingness to take risks, potentially resulting in losses in the context of mixed gambles. We also hypothesized that these risk-averse tendencies would be normalized by levodopa.
MATERIALS AND METHODS
Participants
We tested 36 mildly to moderately affected patients with idiopathic PD and 36 age-matched (±5 years) healthy controls (Table 1). Patients were recruited from the Movement Disorders clinic at the University of British Columbia. Controls were spouses, friends and family members of the patients. The study was approved by the research ethics board of the University of British Columbia and carried out in accordance with the Declaration of Helsinki. Participants gave written informed consent.
Participant demographics and clinical characteristics
Patients were on levodopa monotherapy, with a mean daily dose of 639.58 ± 272.91 mg, ranging from 300 - 1500 mg. Exclusion criteria for both patients and controls were: other central neurological disorders, Montreal Cognitive Assessment (22) score < 24 OFF medication, Beck Depression Inventory (Beck et al., 1961) scores > 14, or ongoing treatment with antidepressants. Participants were characterized dimensionally using the Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease (24), Canadian Problem Gambling Index (25) and Temperament and Character Inventory (26) as a measure of novelty seeking (Table 1). Given the nature of the study and the tasks, participants were excluded for scores suggesting problematic gambling. One control whose questionnaire scores indicated problems with gambling and one patient treated with a low dose of ropinirole (1mg daily) and were excluded from the analyses; including these data influenced the findings. The Unified PD Rating Scale (UPDRS-III, (27)) scores were taken from the clinic database; the mean interval between the date of testing and UPDRS-III administration was 403 ± 512.4 days.
Procedure
Patients were randomly assigned to one of two testing orders: 1) first session OFF, second session ON or 2) first ON, second OFF. For the OFF session, medication was withheld overnight, with the last dose at least 12 hours prior to the experiment for immediate release and at least 18 hours for controlled release levodopa. The two sessions were no more than one week apart. Controls were also tested twice within one week. For the analyses, each control was matched to one PD patient, and their two testing sessions were given ON and OFF labels matching those of the PD patient, even though controls did not receive levodopa.
For the tasks described below, participants played to earn cash bonuses, up to $70 over the two sessions. The tasks were programmed in Experiment Builder (SR Research Ltd, Kanata, ON), and their order was pseudorandomized and matched between patients and controls.
Vancouver Gambling Task
On each trial, participants chose between two prospects: one featuring a larger and less probable gain and the other featuring a smaller and more probable gain (Figure 1A). There were 10 different prospect pairs, each repeated in 10 trials, for 100 trails total. The difference in expected value (i.e. probability x magnitude of reward) between the two prospects in each pair ranged widely, from pairs that highly favored the smaller more probable prospect (the safer option) to pairs that highly favored the larger less probable prospect (the riskier option), as well as pairs that were close in expected value. The probability of gain for the two prospects always added up to one (0.2 / 0.8; 0.3 / 0.7; and 0.4 / 0.6), and reward magnitudes ranged from one to five tokens. Thus, each pair thus had an Expected Value Ratio (EVR) computed as EV(safe) – EV(risky)/mean(EV(safe), EV(risky)) (19). After each choice, the program determined the outcome of the wager based on its stated probability, and participants were given feedback as shown in Figure 1A.

A) Vancouver Gambling Task (VGT); B) Vancouver Roulette Task (VRT). On the VRT, the green portion of the ring represents the probability of winning, the black portion represents the probability of losing, and the number in the centre of the ring is the multiplier.
Vancouver Roulette Task
This assessed the valuation of gains versus losses by asking participants to either accept or reject mixed gambles (Figure 1B). The gambles differed in the balance of the probability of gain versus the probability of loss, which always added up to one. If the participant accepted the gamble, they could bet one, two or three tokens. In the case of a win, the participant received the marginal return on the bet multiplied by a factor that also varied across trials (marginal return = bet*multiplying factor – bet). In the case of a loss, the participant lost the amount they bet. There were 17 different prospects, whose expected values were determined by the probability of gain versus loss and the size of the multiplying factor and ranged from highly favoring the gamble’s acceptance to highly favoring its rejection. Participants completed five blocks of 23 trials, for a total of 115 trials.
Participants were given $10 at the start to offset possible losses.
Participants additionally performed a task of decision making under ambiguity as part of a larger study, which we report in the Supplement. We did not have specific hypotheses regarding performance of this group of levodopa-treated patients of this task.
Statistical Analyses
Demographic and clinical characteristics were analyzed using independent t-tests for continuous and chi square tests for categorical variables. The main analyses were performed using linear mixed effects models implemented via the lme4 package in R (28).
For the Vancouver Gambling Task, we first examined the effects of medication state on the likelihood of taking risks. We used a linear mixed effects model (glmer function) with a logistic link to model safe vs. risky choice on a trial-by-trial basis as a function of medication (ON vs. OFF or corresponding sessions in controls) in interaction with group (PD vs. controls) with both terms as fixed effects. Random intercepts were included for participants, and random slopes were used for the effect of medication.
We then examined the effect of medication in the PD group alone in interaction with gamble characteristics, namely relative expected values of the two prospects (EVR), probabilities and magnitudes. Because probabilities and magnitudes of the two alternatives were evaluated relative to each other, we performed isometric log ratio transformations to derive a single value for each representing relative probabilities and magnitudes of the alternatives. These relative probability and magnitude values were modeled as fixed effect terms in interaction with medication. The random effect structure was the same as above.
Finally, we ran separate models for the OFF and ON states to compare the likelihood of risky choice as a function of gamble characteristics between PD vs. control participants. EVR, probability and magnitude were modelled as fixed effects, and random intercepts were included for participants.
For the Vancouver Roulette Task we modelled three variables describing participants’ choices: 1) accepting vs. rejecting a gamble; 2) betting 2 or more tokens; 3) betting 3 tokens. These decisions were modelled on a trial-by-trial basis using linear mixed effects models with a logistic link, first as a function of group and medication, then using separate models in PD patients and controls to examine the effects of gamble characteristics in interaction with medication, as well as models examining the effects of these characteristics in interaction with group. The random effect structure was same as with the other task.
Gender, age and task order were initially included as terms in all the models but were subsequently dropped as they did not significantly predict any outcomes of interest or improve the fit of the models.
As mentioned earlier, neither task required reinforcement learning. However, because feedback regarding gamble outcomes was provided on a trial-by-trial basis, and effects of implicit reinforcement learning on choice could not be precluded, we additionally examined the effects of outcome history on choice, and these exploratory analyses and results are reported in the Supplement.
RESULTS
Participant Characteristics
Demographics and clinical characteristics for the final analyzed sample are given in Table 1. Patients and controls did not differ significantly on any demographic characteristics. Although none of the participants were clinically depressed, PD patients had significantly higher BDI scores (p=0.03).
Vancouver Gambling Task
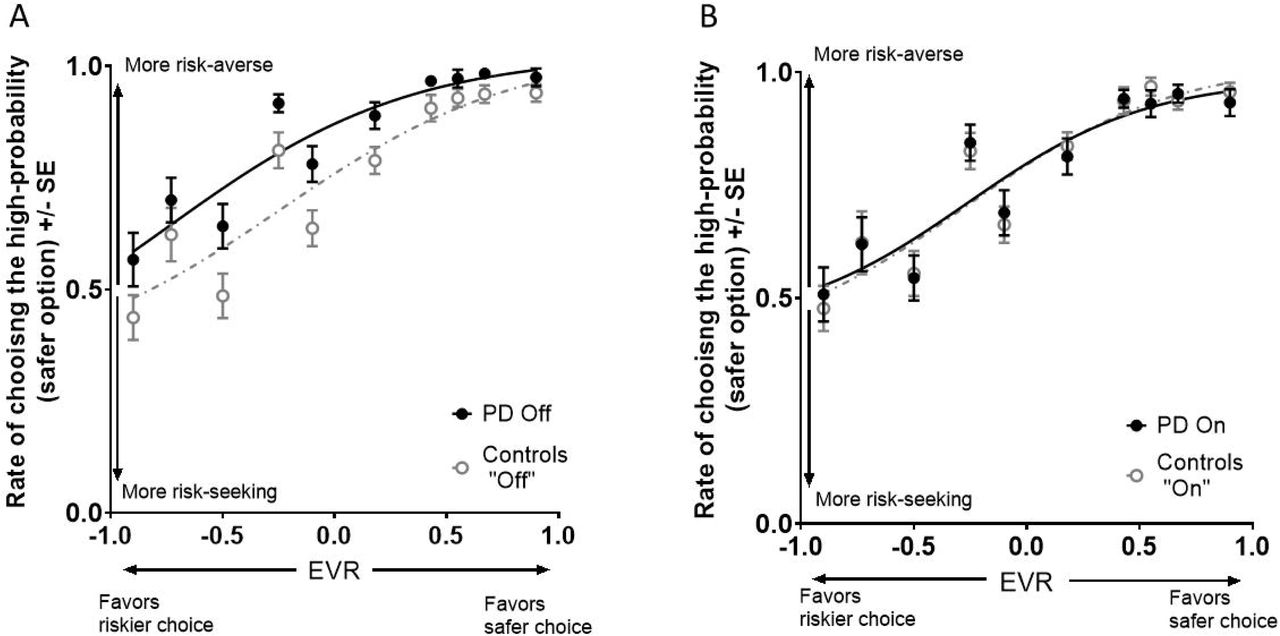
There was a significant interaction between medication and group that predicted the likelihood of choosing the safer versus the riskier prospect (b = 0.58, SE = 0.26, z= 2.27, p = 0.02). The interaction was due to a difference in risk-taking between controls and PD patients in the OFF state but not the ON state (Figure 2). While the choices of PD patients in the ON state did not significantly differ from those of controls (p = 0.78), patients in the OFF state were more risk-averse than controls (main effect of group: b = 0.66, SE = 0.28, z= 2.32, p = 0.02). As expected, controls showed no change in performance from the OFF state-corresponding session to the ON state-corresponding session (p = 0.41). However, PD patients were significantly more likely to take risks in the ON than the OFF state (main effect of medication: b = 0.45, SE = 0.22, z= 2.08, p = 0.04). This medication effect did not interact with EVR, probability or magnitude (ps ≥ 0.11): thus, medication resulted in riskier choice independent of prospect characteristics.

A) Vancouver Gambling Task performance off medication: PD vs. controls; B) VGT performance on medication PD vs. controls. Curves are fitted using a 4-parameter logistic function.
However, there were significant interactions of group with gamble characteristics in both OFF and ON states; we, therefore, report the results collapsed across the medication states. The interactions indicated that the patients’ choices were more driven than those of controls by the gambles’ probabilities (b = 1.03, SE = 0.27, z= 3.81, p = 0.0001); magnitudes (b = 0.52, SE = 0.15, z= 3.44, p = 0.0006); and expected values (b = 0.41, SE = 0.01, z= 4.09, p <0.0005).
In summary, PD patients were risk-averse OFF medication. Levodopa normalized their decision making, resulting in more risk tolerant decisions. Regardless of the medication, patients’ choices were more strongly determined by the expected values of the prospects.
Vancouver Roulette Task
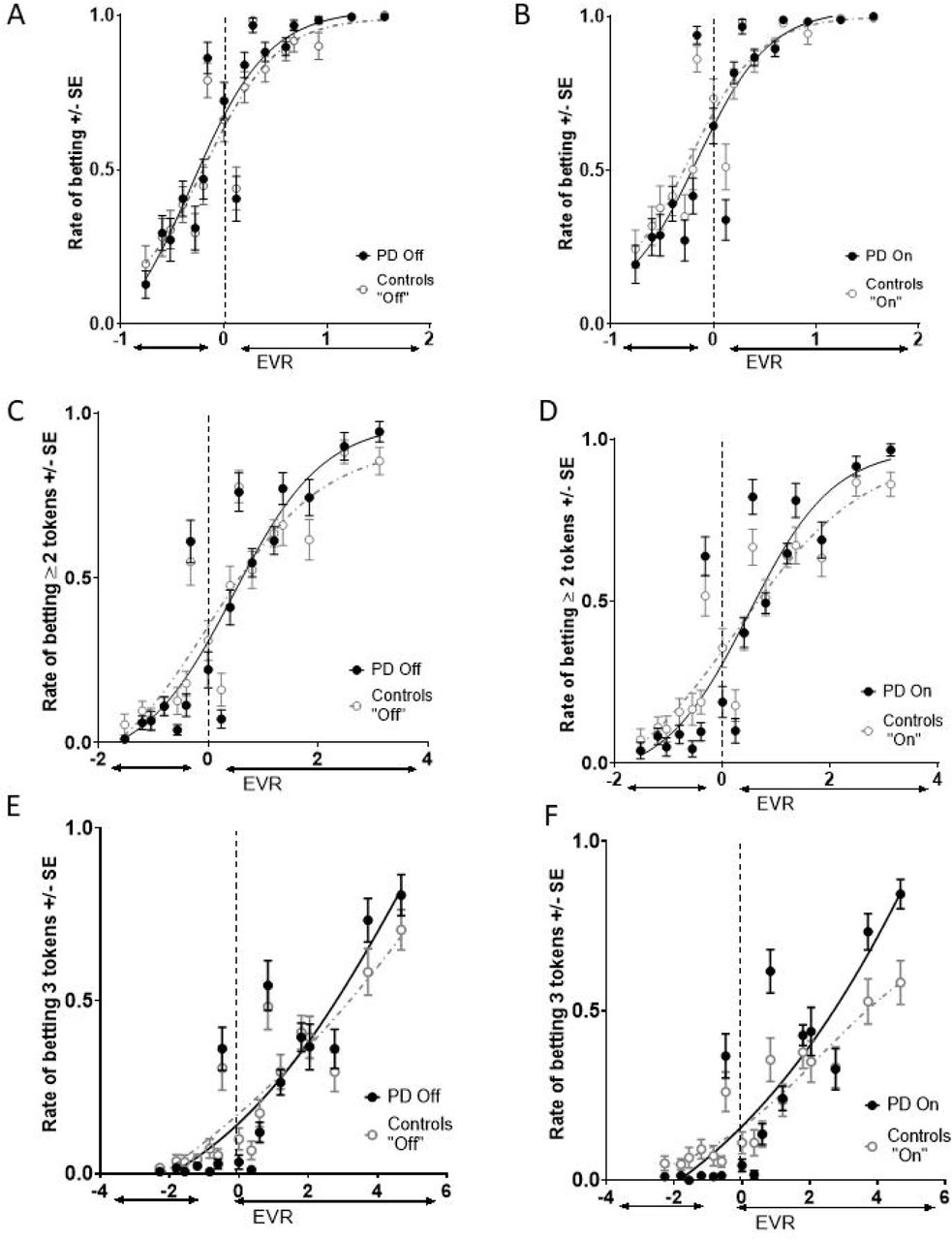
The interaction of group and medication state did not significantly predict the likelihood of accepting the gamble (p = 0.11), nor was there a main effect of group (p=0.29). Both controls and PD patients, whether in the ON or OFF state, disadvantageously accepted gambles with expected values < 0, in which losses were more likely or larger than gains (Figure 3 A&B), indicating a bias to accept rather than to reject an opportunity to bet. PD patients and controls also did not differ in their willingness to place higher bets of 2 or 3 tokens in either OFF or ON state (ps ≥ 0.21).
{kind=link}
{kind=link}
{kind=link}
Rate of betting at least 1 token on the Vancouver Roulette Task as a function of the expected value (EV) of betting 1 token for PDs in the OFF state vs. controls (A) and PDs in ON state vs. controls (B). Rate of betting at least 2 tokens on the VRT as a function of the expected value (EV) for PDs in the OFF state vs. controls (C) and PDs in ON state vs. controls (D). Rate of betting 3 tokens on the VRT as a function of the expected value (EV) for PDs in the OFF state vs. controls (E) and PDs in ON state vs. controls (F).
However, similar to the Vancouver Gambling Task, the patients’ likelihood of betting was more driven than that of controls by prospect characteristics, as evidenced by a significant interaction of group with gain/ loss probability (b = 2.30, SE = 0.55, z=4.23, p < 0.0005), size of the multiplier (b = 1.1, SE = 0.04, z=25.35, p < 0.0005) and the gamble’s expected value computed as the difference between the EV of gain and the EV of loss (b = 4.2, SE = 0.11, z=39.81, p < 0.0005). This was also the case for the likelihood of placing higher bets: there was a significant interaction of group with gain/loss probability (≥2 tokens: b = 4.16, SE = 0.39, z=10.56, p < 0.0005; 3 tokens: b = 6.16, SE = 0.45, z=13.53, p < 0.0005) and the gamble’s expected value (≥2 tokens: b = 0.24, SE = 0.05, z=4.91, p < 0.0005; 3 tokens: b = 0.21, SE = 0.03, z=6.26, p < 0.0005), though not the size of the multiplier. This is reflected in the steeper slope of the patients’ betting likelihood function (Figure 3).
In addition, there was a significant main effect of “medication” collapsing between the groups (b = 0.29, SE = 0.14, z=2.05, p < 0.04), which was driven by the effect of testing session in controls (b = 0.31, SE = 0.14, z=2.25, p < 0.02); this effect was not significant in the patient group. An exploratory analysis showed that the effect in controls was not due to a practice effect (e.g. participants being more risk tolerant or averse in session 1 versus session 2; p=0.99).
In summary, on the Vancouver Roulette Task both PD patients and controls displayed a bias to accept bets with EV < 0. While PD patients and controls did not differ in their overall willingness to bet different amounts, PD patients’ betting behaviour was more driven by probability of gain vs. loss and expected value of a bet.
DISCUSSION
We found evidence of risk aversion for gain-only gambles in unmedicated PD patients relative to matched controls, not attributable to reinforcement learning deficits. The limited evidence of this from previous studies suggests that the risk aversion of PD patients may only manifest under specific experimental conditions. It is currently unclear what these may be, but the discrepancy between the current findings and those using an earlier version of the Vancouver Gambling Task (19) points to the importance of prospect representation. Sharp et al. represented probabilities numerically and magnitudes using square tokens and failed to find OFF state risk aversion in the gain frame, though this study did find risk aversion in the loss frame: patients showed a stronger preference than controls for smaller more likely losses versus larger less likely ones. Numeracy research suggests that neurotypical adults have difficulties with ratio concepts such as probabilities (29), and our own research in young healthy controls using the Vancouver Gambling Task suggests that concrete (pictorial) versus symbolic (numeric) representation of prospective rewards at the time of choice influences willingness to take risks of this task in a value-dependent manner (30). Numeracy challenges may have masked risk aversion of PD patients in the gain frame, which was perhaps more apparent in the loss frame, because unmedicated patients are more sensitive to punishments. As the current study did not measure decision making in the loss frame, and it remains unclear whether the patients’ risk OFF state risk aversion manifests equally in the loss frame.
The patients’ risk aversion on the Vancouver Gambling Task was normalized by levodopa. This medication-induced risk enhancement was value-independent, a result that echoes a recent finding in a mixed sample of patients treated with levodopa and/ or dopaminergic agonists, which increased the patients’ willingness to accept mixed gambles in a value-independent manner (17). Other studies, however, suggested value-dependent effects (15)(16). While the former is in keeping with levodopa increasing value-independent gambling propensity in healthy volunteers (31)(32), the latter is consistent with the effects of dopaminergic therapy on outcome valuation in PD (33). Differences in the ON state, sometimes achieved using levodopa alone and other times combined with dopamine agonists in variable mixtures in patients treated with both levodopa and agonists may have contributed to the variance in findings.
We did not observe loss aversion in PD patients with the mixed prospect design of the Vancouver Roulette Task, nor did we see an effect of medication. Indeed, there was a bias in both patients and controls towards betting even when the expected value of doing so was unfavorable. This bias may have resulted from either a) a house money effect, as participants were given $10 to play with at the outset, b) possible concern that frequent skipping of trials may be construed as poor participation or c) a framing effect, in which skipped trials may have been viewed as missed opportunities. The absence of loss aversion in the patients is in keeping with previous studies (18)(19)(17).
Finally, we observed an increased value-dependence of choice in the PD patients relative to controls regardless of medication state. Thus, the decisions of the patients were more strongly driven by gamble characteristics determining their expected values, while the choices of controls were more stochastic. This, to our knowledge, is a novel finding whose underlying mechanisms remain unclear. A supplemental exploratory analysis looking at the effects of feedback history (streaks of wins and losses) on choice suggested that although choices of controls tended to be more susceptible to feedback history effects (perhaps owing to implicit reinforcement learning), this could not fully account for their choices being more stochastic (see Supplement). Further studies are needed to clarify the clinical and neurobiological significance of increased value-dependence of choice in PD patients.
Our study had limitations. First, we did not obtain UPDRS-III ratings in the ON and OFF sessions. The ratings provided here were taken from our clinic’s database and were dated for some of the participants, and the disease staging data given in Table 1 may not be entirely accurate. This important to consider, as differences in patient samples might contribute to finding inconsistencies across studies of decision making in PD. Secondly, although our mixed gamble Vancouver Roulette Task appears to have face validity and appears to captures age-related changes in risky decision making (34), it did not elicit loss aversion in either patients or controls. Hence, it is possible that differences between patients and controls in valuation of losses relative to gains could have been detected with a more sensitive measure of loss aversion.
In conclusion, this study demonstrated that 1) PD patients are risk-averse for gains without evidence of loss aversion; 2) their risk aversion likely results from dopamine deficiency, as it is normalized by levodopa; 3) patients’ decision making is more value-driven, which may not directly result from dopamine deficiency, as it is independent of medication. This pattern of results points to the role of dopaminergic deficiency in risk aversion in PD, as well as dopamine-independent alterations in other aspects of decision making, such as value-dependence of choice.
Authors’ Roles
Mariya V. Cherkasova: project execution, statistical analysis, manuscript writing
Jeffrey C. Corrow: project execution, manuscript writing
Alisdair Taylor: project organization and execution
Shanna C. Yeung: project execution
Jacob L. Stubbs: project execution and manuscript review and critique
A. Jon Stoessl: project organization and manuscript review and critique
Martin J. McKeown: project organization and manuscript review and critique
Silke Appel-Creswell: project organization
Jason J. S. Barton: project conception, organization, statistical analysis review, manuscript review and critique
Financial Disclosures of all authors (for the preceding 12 months)
Mariya V. Cherkasova: holds funding from the National Center for Responsible Gaming and has received a speaker’s honorarium from the Responsible Gaming Association of New Mexico.
Jeffrey C. Corrow: None
Alisdair Taylor: None
Shanna C. Yeung: received the Craig R Williams (Loblaws) Scholarship and Canadian Medical Hall of Fame/Great-West Life and Canada Life Scholarship in 2018.
Jacob L. Stubbs: None
A. Jon Stoessl: Has received consulting fees from Cellular Dynamics International, speaker and consulting fees from AbbVie and chairs a DSMB for Voyager Therapeutics.
Martin J. McKeown: has received honoraria from Abbvie and Sunovion Pharmaceuticals.
Silke Appel-Cresswell: is supported by the Marg Meikle Professorship for Parkinson’s disease; Research support from Pacific Parkinson’s Research Institute, Weston Foundation, Canadian Consortium on Neuro-degeneration and Aging, Parkinson Canada and CIHR; Travel support and honoraria for speaking and consulting from Allergan, Ipsen, Merz, and Sunovion
Jason J. S. Barton: None
REFERENCES




