

Abstract
16p11.2 and 22q11.2 Copy Number Variants (CNVs) confer high risk for Autism Spectrum Disorder (ASD), schizophrenia (SZ), and Attention-Deficit-Hyperactivity-Disorder (ADHD), but their impact on functional connectivity (FC) networks remains unclear.
We analyzed resting-state functional magnetic resonance imaging data from 101 CNV carriers, 755 individuals with idiopathic ASD, SZ, or ADHD and 1,072 controls. We used CNV FC-signatures to identify major dimensions contributing to complex idiopathic conditions.
CNVs had large mirror effects on FC at the global and regional level, and their effect-sizes were twice as large as those of idiopathic conditions. Thalamus, somatomotor, and posterior insula regions played a critical role in dysconnectivity shared across deletions, duplications, idiopathic ASD, SZ but not ADHD. Individuals with higher similarity to deletion FC-signatures exhibited worse behavioral and cognitive symptoms. These seemingly distinct neuropsychiatric mutations showed similar gene co-expression patterns and converged on FC dimensions, that may represent mechanistic building blocks shared across idiopathic conditions.
Introduction
Copy number variants (CNVs) are deletions or duplications of DNA segments and represent an important source of genetic variation. An increase in rare CNV burden has been linked to a range of neurodevelopmental and psychiatric conditions 1,2. Twelve recurrent CNVs have been individually associated with autism spectrum disorder (ASD) 3, eight with schizophrenia (SZ) 4, and eight with attention deficit hyperactivity disorder (ADHD) 5 but the mechanisms by which they lead to neuropsychiatric disorders remain unclear. Although they have large impacts on neurodevelopment, their effect alone does not lead to a psychiatric diagnosis. CNVs could therefore be leveraged to identify major dimensions contributing to complex idiopathic conditions.
CNVs at the proximal 16p11.2 and 22q11.2 genomic loci are among the most frequent large effect-size genomic variants and alter the dosage of 29 and 50 genes, respectively 6,7. They confer high risk for ASD (10-fold increase for the 16p11.2 deletion and duplication) 3, SZ (>10-fold increase for the 22q11.2 deletion and 16p11.2 duplication) 4, and ADHD 8–12. Gene dosage (deletions and duplications) affect the same neuroimaging measures in opposite directions. Structural alterations of the cingulate, insula, precuneus and superior temporal gyrus overlap with those observed in meta-analytical maps of idiopathic psychiatric conditions including ASD and SZ.10,11
Large effect-size mutations can shed light on pathways connecting genetic risk to brain endophenotypes, such as functional connectivity (FC). However, few studies have investigated the effect of ‘neuropsychiatric’ CNVs on FC. Dysconnectivity of thalamic-hippocampal circuitry 13 has been reported in 22q11.2 deletion carriers, with prominent under-connectivity of the default mode network (DMN), which was predictive of prodromal psychotic symptomatology 14,15. Impaired connectivity of long-range connections within the DMN has also been reported by other studies 16. A single 16p11.2 study has showed a decrease in connectivity of fronto-temporal and -parietal connections in deletion carriers 17. These initial studies have focussed on regions of interest but connectome-wide association studies (CWAS) analysing all connections without a priori hypotheses have not yet been performed in CNV carriers. Furthermore, their relation with idiopathic conditions has not been investigated.
Brain intermediate phenotypes of psychiatric conditions, have mainly been studied by adopting a top-down approach, starting with a clinical diagnosis and moving to underlying neural substrates and further down to genetic factors 18. Studies applying this strategy in ASD have shown reproducible patterns of both over-connectivity (prefrontal and parietal cortices) and under-connectivity (sensory-motor regions) 19. In contrast, SZ patients tend to exhibit a general under-connectivity profile, mainly involving the medial prefrontal cortex, the cingulate and the temporal lobe 20, with the exception of over-connectivity of the thalamus 21. These altered networks do not appear to be disorder-specific and have been reported across several disorders, including ASD, ADHD, and SZ 22. These similarities seem to be distributed across several continuous dimensions 23 which may be related to shared genetic contribution across diagnoses, which is documented for common 24 and rare 25 variants, including the 16p11.2 and 22q11.2 CNVs.
We posit that seemingly distinct genetic variants and idiopathic disorders have overlapping patterns of dysconnectivity, which may help identify FC dimensions, providing insight into the complex connectivity architecture involved in psychiatric conditions.
We aimed to 1) characterize the FC-signatures of four high-risk neurodevelopmental CNVs and 2) explore whether FC-signatures of CNVs represent dimensions observed in idiopathic ASD, SZ, or ADHD.
To this end, we performed CWAS studies on 101 carriers of a 16p11.2 or 22q11.2 CNV, 122 of their respective controls, 751 individuals with idiopathic ASD, SZ, or ADHD and 948 of their respective controls. To our knowledge, this is the first connectome-wide study to compare rare genomic variants and idiopathic psychiatric conditions.
Results
16p11.2 and 22q11.2 CNVs have large effects on functional connectivity at the global and regional level
The 16p11.2 deletion showed a global increase in FC of 0.31 z-scores (based on the variance of the respective control group, Supplementary Table S1.1) when compared with control subjects (p=0.011, permutation test, Figure 1a,c). We observed over-connectivity in 88 connections (FDR, q < 0.05), with beta values ranging from 0.76 to 1.34 z-scores. Overconnectivity predominantly involved the fronto-parietal, somatomotor, ventral attention, and basal ganglia networks (Figure 1c). Regions showing the strongest mean connectivity alterations included the caudate nucleus, putamen, lateral frontal pole, anterior middle frontal gyrus, and dorsal anterior cingulate cortex (Supplementary Table S1.8).

(a-b): Scatterplot (hexagonal plot), showing estimates (beta values) from connectome-wide association studies (CWAS) performed between 16p11.2 (a) and 22q11.2 (b) CNVs and their respective controls. In total, 2,080 beta estimates were obtained from a linear model computed from z-scored connectomes based on the variance of the respective controls. The color hue represents the number of beta estimates in the hexagon bin. Y axis: beta values associated with deletions (CWAS comparing deletions vs controls). X axis: beta-values associated with duplications (CWAS comparing duplications vs controls).
(c-d): Each chord diagram shows the top 20% of connections surviving FDR correction (q < 0.05) from the 16p11.2 deletion (c) and 22q11.2 deletion (d) CWAS. Each chord represents a significantly altered connection between two functional seed regions. All 64 seed regions are represented in the dark grey inner circle. The width of the seed region in the grey inner circle corresponds to the number of altered connections. Seed regions are grouped into 12 functional networks (outer ring, Supplementary Table S1.9). Networks are represented in 12 brains below the two diagrams. Red chords represent overconnectivity and blue chords underconnectivity.
The 22q11.2 deletion was associated with a global decrease in connectivity (z-scores = −0.25, Supplementary Table S1.3), with 68 connections surviving FDR correction (beta values ranging from −0.59 to −1.69 z-scores, Figure 1b, d). Underconnectivity predominantly involved the anterior and lateral DMN, and limbic network (Figure 1d). The temporal pole, the ventral anterior insula and peri-insular sulcus, the amygdala-hippocampal complex, the dorsal anterior cingulate cortex, and perigenual anterior cingulate cortex showed the strongest changes in connectivity (see Supplementary Table S1.8).
16p11.2 duplication carriers showed a mean reduction of connectivity (z-score = −0.25, Figure 1a and Supplementary Table S1.2) relative to controls (p = 0.034, permutation test), but none of the individual connections survived FDR correction. A sensitivity analysis showed that results are unaffected by differences in age distribution between deletions and control groups (see Supplementary Results).
22q11.2 duplications showed an overall increase in connectivity (z-score = 0.23, Figure 1c and Supplementary Table S1.4), but only 16 connections survived FDR correction involving the posterior medial and lateral visual network, the cerebellum I-V, and the lateral fusiform gyrus (see Supplementary Table S1.8).
Deletions and duplications at both loci showed a mirror effect at the global connectivity level. 16p11.2 deletions and duplications also showed mirrors effects at the network level (p = 0.006, two-sided). This was not the case for 22q11.2 (Supplementary Results).
The effect sizes of deletions and duplications are twice as large as the effects of idiopathic SZ, ASD, or ADHD
We performed three independent CWAS, comparing FC between patients with ASD, SZ, ADHD, and their respective controls. Idiopathic SZ showed overall underconnectivity affecting 835 connections, in line with previous reports 21,26 (Figures 3a, 3c, Supplemental Results and Tables S1.6 and S1.8). Over-connectivity was restricted to 24 connections (FDR, q < 0.05).
Idiopathic ASD also showed overall underconnectivity (73 under and 2 overconnected survived FDR, q < 0.05, Figure 3b, 3c, Supplemental Results and Tables S1.5 and S1.8).
For ADHD, none of the individual connections survived FDR correction (Supplemental Results and Tables S1.7 and S1.8). Sensitivity analyses excluding females from the SZ and ADHD cohorts showed identical results (Supplementary Results).
Among idiopathic conditions, the effect size of connectivity alteration was the highest in SZ (largest beta value = −0.56 std of the control group), followed by autism (largest beta value = −0.46), and ADHD (largest beta value = +0.26). Effect sizes observed for both deletions were approximately two-fold larger (beta values = +1.34 and −1.69 for 16p11.2 and 22q11.2 respectively) than those observed in idiopathic SZ, ASD, and ADHD (Figure 3c). The largest effect size among the 16 connections surviving FDR for the 22q11.2 duplication was Cohen’s d= 1.87.
Individuals with ASD and SZ relative to controls, show similarities with whole brain FC-signatures of CNVs
We tested the spatial similarity between whole-brain FC-signatures across CNVs and idiopathic psychiatric conditions. To this mean we computed the similarity (Pearson R) between group level FC-signatures, and the individual connectomes of either cases or controls from another group (Figure 2). This was repeated 42 times between all CNVs and conditions and in both directions. Most of the significant whole brain FC similarities were observed between individuals with either idiopathic ASD, SZ and 4 CNVs (Figure 3d). ADHD did not show any significant similarities with any other group.
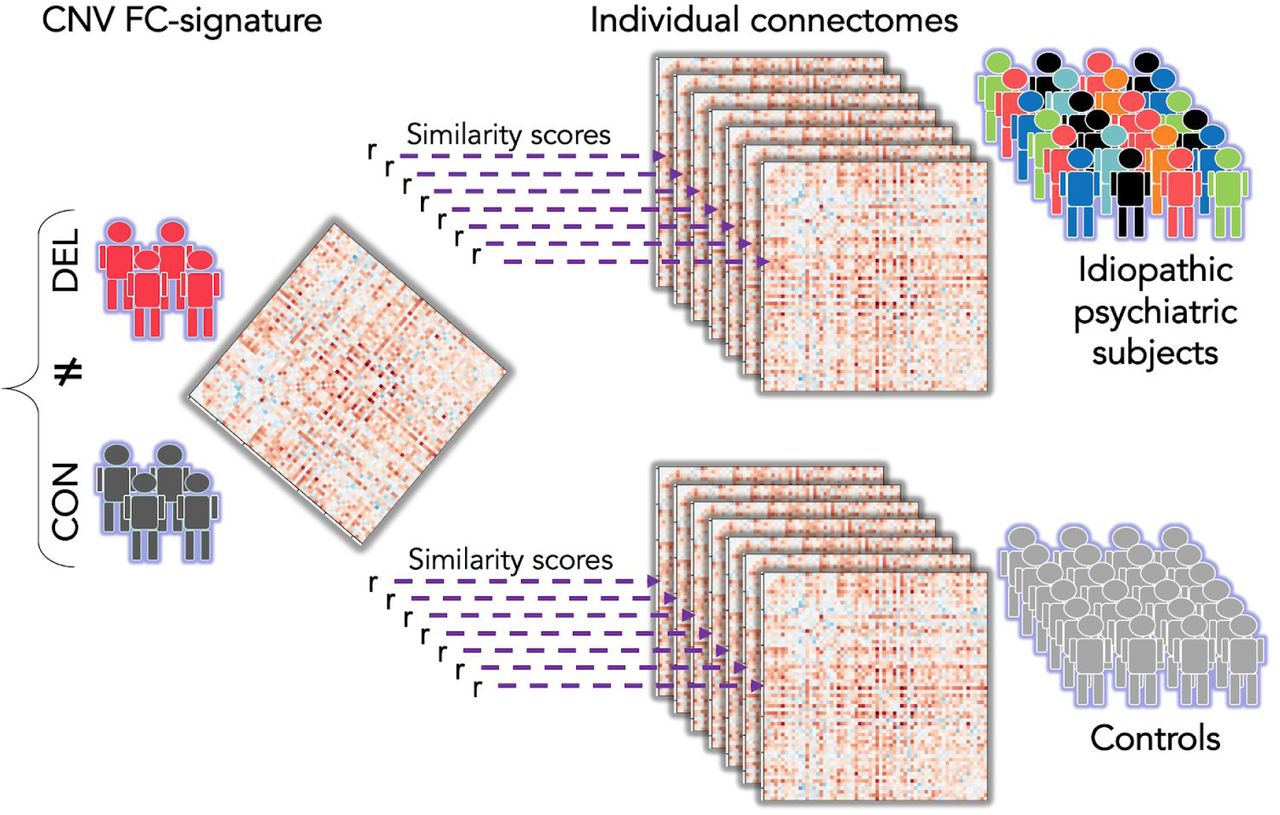
Similarities of FC-signatures across this study were characterized by correlating (Pearson’s r) a group level FC-signature with individual connectomes from either cases and controls. The r values obtained for all cases and all controls were compared using a Mann Whitney test. Here, the group level connectome is represented by a matrix of 2080 beta values, on the left side. It is obtained by contrasting deletion cases (red) and controls (dark grey). The beta map is correlated to 7 individual connectomes of psychiatric cases and 7 connectomes of controls. The different colors used for the psychiatric cases represent phenotypic heterogeneity.
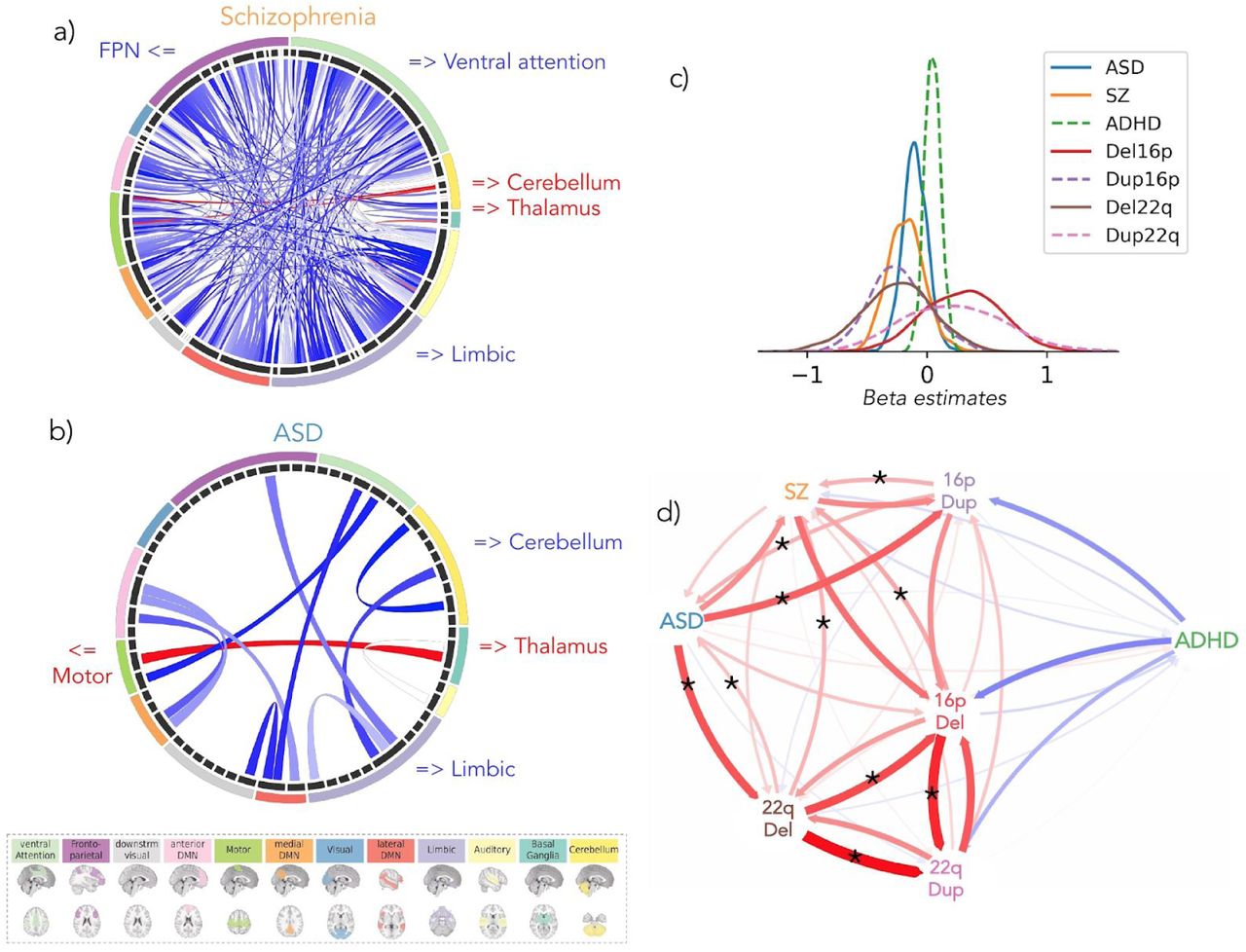
(a, b): Each chord diagram shows the top 20% connections surviving FDR correction (q < 0.05) from the SZ (a) and ASD (b) CWAS. Each chord represents a significantly altered connection between two functional seed regions. All 64 seed regions are represented in the dark grey inner circle. The width of the seed region in the grey inner circle corresponds to the number of altered connections. Seed regions are grouped into 12 functional networks (outer ring, Supplementary Table S1.9). The network colors correspond to the legend below. Red chords represent overconnectivity and blue chords underconnectivity. (c) Density plots represent the distribution of 2080 beta estimates for the CWAS (whole brain contrast of cases versus controls) for the SZ, ASD, ADHD, deletion and duplication groups. X axis values = z-scores of Beta estimates, which were obtained from linear models computed using z-scored connectomes based on the variance of the respective controls. (d) Spatial similarity of whole-brain FC-signatures between CNVs and idiopathic psychiatric conditions. Arrows represent the correlation between group level FC-signatures, and the individual connectomes of either cases or controls from another group. The correlation was computed in both directions. Red and blue arrows represent positive and negative correlations respectively. Arrow thickness represents the effect size of the Mann-Whitney test. Stars represent similarities (Mann-Whitney tests) surviving FDR.
ASD: autism spectrum disorder; SZ: schizophrenia; ADHD: attention deficit hyperactivity disorder; FPN: fronto-parietal network; 16pDel: 16p11.2 deletion; 22qDel: 22q11.2 deletion, 16pDup: 16p11.2 duplication; 22qDup: 22q11.2 duplication
Thalamus and somatomotor regions play a critical role in dysconnectivity observed across CNVs and idiopathic psychiatric conditions
We asked if whole brain FC similarities between individuals with ASD, SZ and CNVs may be driven by particular regions. We thus repeated the same similarity analysis presented above at the level of the FC signatures of each of the 64 seed regions. Individuals with SZ showed increased similarity with 28 out of the 64 regional FC-signatures of the 16p11.2 deletion than controls (FDR, q < 0.05). They also showed increased similarity with 18 region-level FC-signatures of the 22q11.2 deletion (Figure 4, Supplementary Tables S2.3 and S2.4, and Results). Deletion FC-signatures did not show any similarity with controls. We ranked the effect size of each seed region and compared them for both deletions. The seed regions with the highest similarity between SZ and 16p11.2 were also those with the highest similarity between SZ and 22q11.2 (adjusted R2 = 0.3709, p = 6e-08) (see Supplementary Results).

The FC-signatures of both deletions are decomposed into 64 seed-regions. Deletion FC-signatures are correlated to the individual connectivity profile of subjects with a psychiatric diagnosis and their respective control subjects. Of note, the correlation is equivalent to the mean centering of all region-based FC-signatures. Significantly higher similarities of patients with either ASD and SZ were present in 33 seeds regions (FDR) and are presented on the right and the left side of the diagram, respectively. At the intersection of all ellipses, the thalamus FC-signatures of both deletions showed increased similarity with individuals who have a diagnosis of ASD or SZ compared to their respective controls.
16pDel: 16p11.2 deletion, 22qDel: 22q11.2 deletion; Ant: anterior; Post: posterior; dorsolat: dorsolateral; Inf: inferior; L.: left; v.: ventral; net.: network; med: medial; Supp: supplementary; lob: lobule (Full-name labels are provided in Supplementary Table S1.9).
Individuals with autism showed greater similarity with six regional FC-signatures of the 16p11.2 deletion compared to controls (FDR, q < 0.05). They also showed greater similarity with six region-level FC-signatures of the 22q11.2 deletion (Figure 4, Supplementary Tables S2.1 and 2.2, and Results). Deletion FC-signatures did not show significant similarities with controls for any of the 64 seed regions. Of note, individuals with SZ and ASD showed higher similarity with the thalamus FC-signatures of both deletions (Figure 4). None of the similarities correlated with motion or sex. Regions driving similarities between psychiatric conditions and deletion FC signatures were also those with the highest number of connections altered by each deletion individually. Eight and six out of the top 10 regions altered by 22q11.2 and 16p11.2 respectively were driving similarities with psychiatric conditions (Supplementary Table 1.8).
Despite lower power, we investigated similarities with duplication FC-signatures. The number of significant regional similarities was smaller. Out of the 28 regions showing a similarity between idiopathic conditions and duplications, 17 regions also showed similarities with deletions (See Supplementary Results). Individuals with ADHD, did not show higher similarities with the regional FC-signatures of any CNVs except for 2 regional FC-signatures of the 16p11.2 duplication (Supplementary Tables S2.5 and S2.6).
Similarity to deletion FC-signatures is associated with symptom severity
We investigated whether regional FC similarities with deletions described above are associated with symptom severity among individuals in idiopathic psychiatric cohorts. Symptom severity was assessed using the Autism Diagnostic Observation Schedule (ADOS, 27), in ASD, Positive and Negative Syndrome Scale (PANSS, 28) in SZ, and Full Scale Intelligence Quotient (FSIQ) in ASD. The 10 seed regions with significant FC similarity between ASD and either deletion were those showing the strongest association with the ADOS symptom-severity score (two regions passed FDR correction q < 0.05: the caudate nucleus and temporal pole) and FSIQ (Figure 6 and Supplementary Tables S3.1-3.4). Among the seed regions contributing to the similarity between SZ individuals and deletions, none were significantly associated with PANSS measures after FDR correction. FSIQ data was not available in the SZ cohorts.
16p11.2 and 22q11.2 deletions show regional FC and gene co-expression similarities
Although the two deletions showed opposing effects on global connectivity (Figure 3c), their connectomes were positively correlated (Figure 3.d). We therefore sought to identify the main regions that contributed to this connectome-wide correlation.
Using the same approach as above (Figure 2), we correlated the 22q11.2 deletion group-level FC-signature with individual connectomes of 16p11.2 deletion carriers and their respective controls. The 22q11.2 deletion FC-signature showed significant similarities with 16p11.2 deletion carriers for 12 regions (FDR, q<0.05), mainly involving the fronto-parietal, ventral attentional, and somatomotor networks. The reverse test showed significant similarity of the 16p11.2 deletion FC-signature with 22q11.2 deletion carriers in 10 regions within the anterior and lateral DMN, fronto-parietal and basal ganglia networks. Four seed regions were observed in both tests (Figure 5a).
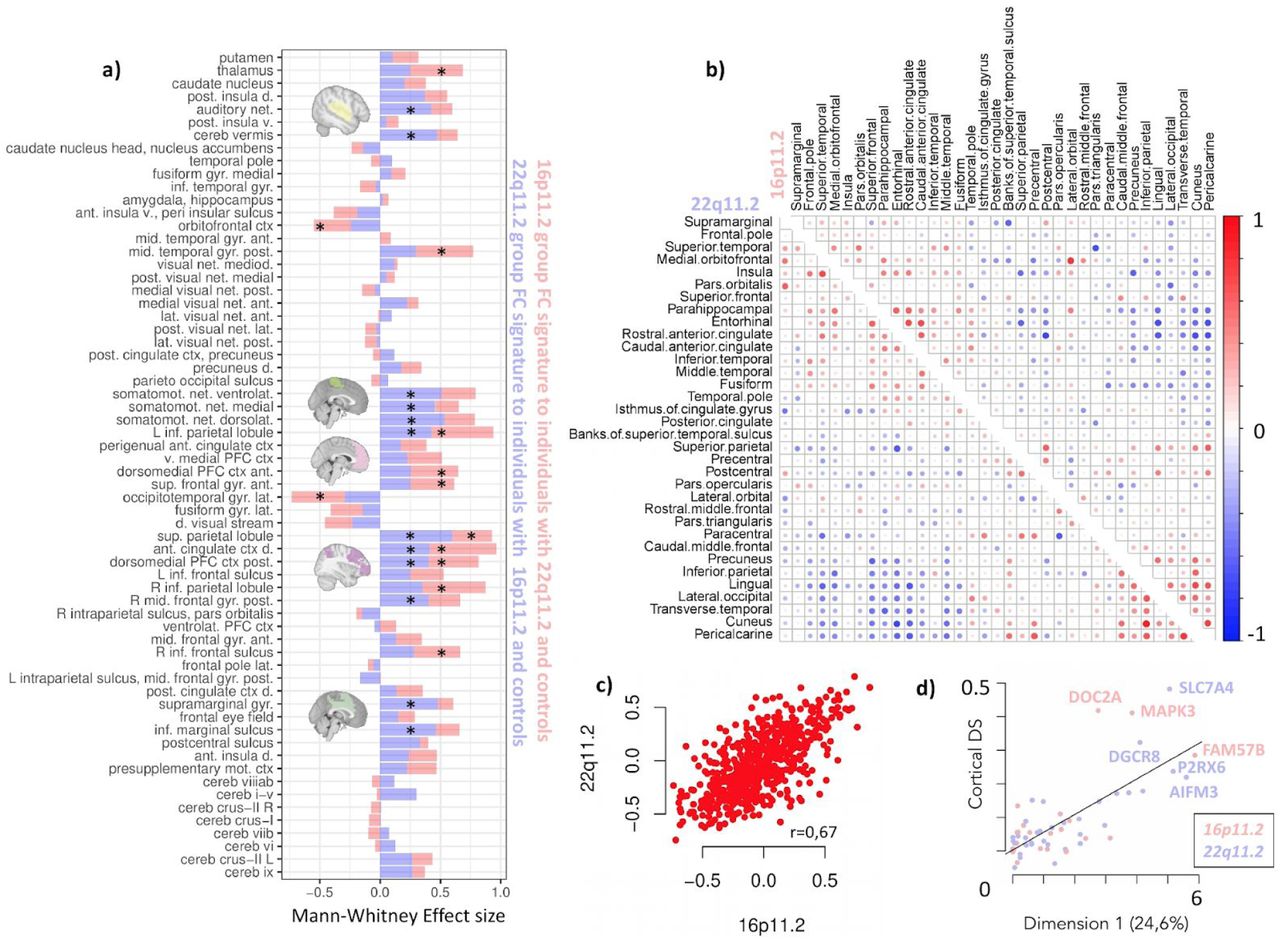
(a) Regional similarity between both deletions. The horizontal axis values represent the Mann whitney effect size (rank biserial correlation). The vertical axis represents the 64 functional regions. Blue bars represent the correlation between the 22q11.2 deletion-FC-signature (at the group level) and individual connectomes of either 16p11.2 deletion carriers or controls. Pink bars represent the reverse test. Stars represent significant similarities (FDR accounting for 64 tests, q<0.05). Full-name labels are provided in Supplementary Table S1.9.
Panel: (b) Two coexpression matrices for genes within the 16p11.2 (upper triangle) and 22q11.2 (lower triangle). We performed hierarchical clustering based on all genes from both genomic loci. Each row and column represents on of the 34 neuroanatomical regions extracted from the Desikan freesurfer atlas. The Pearson R value is represented in the color bar. (c) The 16p11.2 and 22q11.2 co-expression patterns are highly correlated. Each point is a co-expression value. X and Y axes represent co-expression R-values present in the two triangles of the co-expression matrices (b). (d) Genes contributing the most to dimension 1 (variance of gene expression across all regions) are those with the highest cortical DS score 29. Genes contained in the 16p11.2 CNV and 22q11.2 are represented in pink and purple respectively. Y axis= Cortical Differential Stability score (DS). X axis= Contribution in percent to dimension 1.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
a) Boxplots represent the connectivity similarity for two seed regions (thalamus and perigenual anterior cingulate cortex). Each data point represents one individual: r value of the Pearson correlation between the deletion FC-signatures and the FC-profile of an individual with ASD (n = 221 in the colored boxplots) or a control subject (n = 232 in the non-colored boxplots). For the two seed regions, individuals with ASD show significantly higher similarity (FDR, q < 0.05) with the 16p11.2 (pink) and 22q11.2 (yellow) deletion FC-signatures than the individual controls. All seed regions showing significantly higher similarity with ASD are represented in the Venn diagram on the left. b) We investigated the relationship with cognitive scores and found that stronger individual similarity with the deletion FC-signature was associated with more severe symptoms measured by FSIQ and ADOS. Heatmaps show the level of correlation between behaviour scores and the similarity with deletion FC-signatures
16pDel: 16p11.2 deletion, 22qDel: 22q11.2 deletion; FSIQ: full-scale intelligence quotient; ADOS: autism diagnostic observation schedule; ant.: anterior; post: posterior; v.: ventral; PFC: prefrontal cortex; cereb: cerebellum; d.: dorsal; L: left; ctx: cortex; net.: network. (Full-name labels are provided in Supplementary Table S1.9).
We reasoned that the FC-similarity between CNVs may be related to the large-scale transcriptomic organization of genes within both genomic intervals. Gene coexpression analysis using the 22 and 35 genes encompassed in the 16p11.2 and 22q11.2 loci respectively showed similar topological co-expression patterns, which were highly correlated (Pearson R=0.67, CI=[0.64;0.70], Figure 5c, Supplementary Tables S4.1). These co-expression patterns involved visual, limbic and cingulate regions. To identify genes and brain regions driving this topological similarity, we performed a principal component analysis (PCA) of expression levels of all 57 genes (at both loci) across all brain regions. The genes contributing most to dimension 1 were also those with the highest cortical differential stability score (R=0.73, Figure 5d, Supplementary Tables S4.2 andResults). Differential stability score is defined as the tendency for a gene to exhibit reproducible topological pattern of expression across brain structures 29. Top genes contributing to dimension 1 included MAPK3, FAM57B, DOC2A for 16p11.2 as well as, P2RX6, DGCR8, SLC7A4, AIFM3 for 22q11.2. Top regions contributing to dimension 1 included the visual and limbic circuits as well as the anterior cingulate cortex (See Supplemental Results).
Discussion
This proof of concept study provides the first connectome-wide characterization of four CNVs that confer high risk for psychiatric disorders. Deletions and duplications at the 16p11.2 and, to a lesser extent, the 22q11.2 locus were associated with mirror effects at the connectome-wide level. Overconnectivity in the 16p11.2 deletion predominantly involved the ventral attention, motor, and frontoparietal networks. Underconnectivity in the 22q11.2 deletion involved the anterior and lateral DMN and the limbic network. Regional FC signatures of deletions and duplications, in particular, those implicating the thalamus, somatomotor, posterior insula and cingulate regions contributed to the complex architecture of idiopathic ASD, SZ but not ADHD. Seemingly distinct, rare neuropsychiatric mutations may converge on dimensions representing mechanistic building blocks shared across idiopathic conditions. Genes encompassed in both loci showed similar co-expression topological patterns, and may partially explain the convergence of CNVs on shared FC signatures.
22q11.2 and 16p11.2 CNVs had large effect sizes on FC that are similar to those previously reported for structural neuroimaging measures, cognition, and behaviour 8,10,11. In sharp contrast, there is a significant discordance between the severe clinical manifestations observed in idiopathic ASD and SZ, and the small effect-size observed in case-control studies at the FC level. Previous structural neuroimaging studies of the same idiopathic psychiatric conditions have also reported small effect sizes 30,31. This discordance may be due to the heterogeneity of these idiopathic conditions and hints at the presence of subgroups or latent dimensions associated with larger effect sizes 23.
The FC-signatures of both deletions (and to a lesser extent those of both duplications) showed connectome-wide similarities with autism and schizophrenia, but not ADHD. These FC similarities may explain the known association between these CNVs and psychiatric conditions. The connectivity signatures of 33 seed regions were the main contributors to these similarities. Most of these regions were also those with the highest number of connections altered by each deletion individually. The same seed regions also showed the highest association with ASD severity scores and general intelligence in the idiopathic autism sample. Our results highlighted the thalamus and somatomotor regions as key hubs altered across most CNVs and psychiatric groups. The thalamus plays an essential role in controlling the engagement of association networks which might be particularly vulnerable to dysregulations in mental illness 32. Somatomotor networks are central to recently identified FC dimensions altered across psychiatric illnesses 23. The extent to which idiopathic psychiatric disorders show similarities with deletions and duplications, is in line with an emerging body of literature that points to common neurobiological substrates for mental illness 33. Evidence includes the genetic covariance between psychiatric disorders 24,34, pleiotropic effects of CNVs associated with several conditions 2,35, and functional neuroimaging studies showing dysconnectivity shared across psychiatric disorders 22.
Genes encompassed in both genomic regions were organized following highly similar co-expression patterns which may provide clues to FC-similarities between CNVs. Recent work has shown that the brain transcriptome is following broad spatial trends that are closely related to the functional network architecture 36,37.
Functional connectivity studies using a top down case-control approach (eg. autism versus control) have characterize large-scale brain network changes associated with diseases, but this framework is unable to describe the directionality of this relationship 38. FC-changes may not necessarily represent an intermediate brain phenotype but rather a secondary impact of psychiatric illnesses. Our strategy integrating top-down and bottom-up approaches shows that individuals with idiopathic ASD or SZ as well as CNV carriers who do not meet diagnostic criteria for these conditions share regional FC alterations. This suggests that the risk conferred by genetic variants and the associated FC-patterns represent important dimensions that are necessary but insufficient to cause disease. Additional factors and associated FC-patterns are required (incomplete penetrance 39). Bottom-up approaches studying rare variants have almost exclusively been performed individually. Our results suggest, however, that they likely converge on overlapping intermediate brain phenotypes, consistent with a recent study showing overlapping effects on subcortical structures across 12 different CNVs conferring risk to SZ 40.
Limitations
The results on duplications should be interpreted with caution due to our limited power to detect changes in connectivity. The limited phenotypic data in the SZ group did not allow to investigate the relationship between deletion FC-signatures and cognitive traits in this sample. Lack of similarity observed for ADHD is line with the small association between 16p11.2 CNVs and ADHD but is discordant with the association reported for 22q11.2 5. ADHD has a smaller effect size than SZ and ASD, which may have limited our analysis 41. Several confounding factors may have influenced some of the results. Those include sex bias, which is present across all 3 psychiatric cohorts, age differences in the 16p11.2 deletion group, and medication status. However, carefully conducted sensitivity analyses, investigating all of these confounders did not change any of the results. Finally, differences in methodology do not allow to directly compare our findings with a previous report on 16p11.2 deletions 17.
Conclusion
Deletion and duplication at several genomic loci result in mirror effects across many human traits 42–45, including brain connectivity. Haploinsufficiency may define functional connectivity dimensions that represent building blocks contributing to idiopathic psychiatric conditions. The overlap of functional connectivity alterations between different deletions may be due to the shared topological gene co-expression patterns. Our results show that it is becoming increasingly difficult to justify the study of psychiatric conditions or rare genetic variants in isolation. Large scale studies simultaneously integrating a top-down approach across diagnostic boundaries, and a bottom-up investigation across a broad set of genomic variants are required to improve our understanding of specific and common psychiatric outcomes associated with genetic variants and FC signatures.
Materials and Methods
Samples
We performed a series of CWAS using individuals from five data sets (Table 1 and Supplementary Materials and Methods).
Description of the cohorts after filtering for quality criteria. SVIP: Simons Variation in Individuals Project; UCLA: University of California, Los Angeles; ASD: autism spectrum disorder; ABIDE: Autism Brain Imaging Data Exchange; SZ: schizophrenia; ADHD: attention deficit/hyperactivity disorder; Del: deletion; Dup: duplication; Age (in years); FSIQ: Full Scale Intelligence Quotient; M: male; FD: framewise displacement (in mm). Quantitative variables are expressed as the mean ± standard deviation. *More information regarding the remaining number of time frames for each group, and the percentage of motion censoring, is provided in Supplementary Materials and Methods. Sensitivity analyses investigating sex bias in the 3 idiopathic cohorts are presented in Supplementary Results. Sensitivity analysis investigating medication effect in ASD cohort is presented in Supplementary Results.
1-2) Two genetic-first cohort (recruitment based on the presence of a genetic variant, regardless of any DSM diagnosis):
16p11.2 deletion and duplication carriers (29.6-30.1MB; Hg19), and extrafamilial controls from the Simons Variation in Individuals Project (VIP) consortium 46.
22q11.2 deletion and duplication carriers (18.6-21.5MB; Hg19) and extrafamilial controls from the University of California, Los Angeles.
3) Individuals diagnosed with ASD and their respective controls from the ABIDE1 multicenter dataset 47.
4) Individuals diagnosed with SZ (either DSM-IV or DSM-5) and their respective controls. We aggregated fMRI data from 10 distinct studies.
5) Individuals diagnosed with ADHD (DSM-IV) and their respective controls from the ADHD-200 dataset48,49.
Imaging data were acquired with site-specific MRI sequences. Each cohort used in this study was approved by the research ethics review boards of the respective institutions. Signed informed consent was obtained from all participants or their legal guardian before participation. Secondary analyses of the listed datasets for the purpose of this project were approved by the research ethics review board at Sainte Justine Hospital. After data preprocessing and quality control, we included a total of 1,928 individuals (Table 1).
Preprocessing and quality control procedures
All datasets were preprocessed using the same parameters with the same Neuroimaging Analysis Kit (NIAK) version 0.12.4, an Octave-based open source processing and analysis pipeline 50. Preprocessed data were visually controlled for quality of the co-registration, head motion, and related artifacts by one rater (Supplementary Materials and Methods).
Computing connectomes
We segmented the brain into 64 functional seed regions defined by the multi-resolution MIST brain parcellation 51. FC was computed as the temporal pairwise Pearson’s correlation between the average time series of the 64 seed regions, after Fisher transformation. The connectome of each individual encompassed 2,080 connectivity values: (63×64)/2 = 2016 region-to-region connectivity + 64 within seed region connectivity. We chose the 64 parcel atlas of the multi-resolution MIST parcellation as it falls within the range of network resolution previously identified to be maximally sensitive to functional connectivity alterations in neurodevelopmental disorders such as ASD.52
Statistical analyses were performed in Python using the scikit-learn library 53. Analyses were visualized in Python and R. Code for all analyses and visualizations is being made available online through the github platform https://github.com/labjacquemont.
Statistical analyses
All of the following analyses are summarised in Supplemental Materials and Methods.
Connectome-wide association studies
We performed seven CWAS, comparing Functional Connectivity (FC) between cases and controls for four CNVs (16p11.2 and 22q11.2, either deletion or duplication) and three idiopathic psychiatric cohorts (ASD, SZ, and ADHD). Note that controls were not pooled across cohorts. Within each cohort, FC was standardized (z-scored) based on the variance of the respective control group. CWAS was conducted by linear regression at the connectome level, in which z-scored FC was the dependent variable and clinical status the explanatory variable. Models were adjusted for sex, site, head motion, and age. We determined whether a connection was significantly altered by the clinical status effect by testing whether the β value (regression coefficient associated with the clinical status variable) was significantly different from 0 using a two-tailed t-test. This regression test was applied independently for each of the 2,080 functional connections. We corrected for the number of tests (2,080) using the Benjamini-Hochberg correction for FDR at a threshold of q < 0.05 54, following the recommendations of Bellec et al. 2015 55.
We defined the global FC shift as the average of the β values across all 2,080 connections and tested for significant case-control differences in average global FC by a permutation test, shuffling the clinical status labels of the individuals included in each CWAS (using 10,000 replications). For example, we randomly permuted the clinical status of 16p11.2 deletion carriers and their respective controls in the 16p11.2 deletion vs control CWAS. We then estimated a valid permutation-based p-value associated with the observed average FC shift 56.
Gene dosage mirror effects on functional connectivity
We tested whether networks are affected by gene dosage in a mirror fashion by computing the product of the β values obtained in each genetic group contrasts: “Deletions vs Controls” and “Duplications vs Controls” (separately for 16p11.2 and 22q11.2). Negative values indicate mirror effects of deletions and duplications on FC. Positive values indicate effects in the same direction for deletions and duplications. The obtained products of the β values were grouped into 12 canonical functional networks using information from the multi-resolution brain parcellation (Supplementary Table S1.9).
Similarity of whole brain FC-signatures between idiopathic psychiatric conditions and CNVs
We tested the similarity between dysconnectivity measured across idiopathic psychiatric conditions and CNV. This similarity was tested by correlating individual whole brain connectomes of cases and controls of one group to the whole brain FC-signature (group level) of another group (Figure 2). The group-level FC-signature was defined as the 2,080 β values obtained from the contrast of cases vs. controls. This was repeated 21 times between all CNVs and conditions and in both directions (n=42 similarity tests).
Individual connectomes of case and their respective controls were used after independently adjusting for sex, site, head motion, age, and average group connectivity for each of the datasets.
Similarity scores were derived by computing Pearson’s correlations between the whole brain connectomes. We asked whether cases compared to their respective controls had significantly higher (or lower) similarity to whole brain FC-signature of another group using a Mann-Whitney U test. We reported significant group differences after FDR correction accounting for the 42 tests (q < 0.05).
Similarity of regional FC-signatures between idiopathic conditions and CNVs
The same approach described above was performed at the regional level. Each of the 1705 connectomes of individuals with idiopathic psychiatric conditions and their respective controls were independently adjusted for sex, site, head motion, age, and average group connectivity for each dataset. We calculated a similarity score between these individual connectomes and the FC-signatures of the 16p11.2 and 22q11.2 deletions and duplications. The FC-signatures were broken down into 64 region-level FC-signatures and similarity scores were derived by computing Pearson’s correlations between the 64 β values associated with a particular region. For each region, we tested whether individuals with a psychiatric diagnosis had significantly higher (or lower) similarity to 16p11.2 or 22q11.2 deletion FC-signatures than their respective controls using a Mann-Whitney U test. We reported significant group differences after FDR correction (q < 0.05) for the number of regions (64).
We investigated the relationship between symptom severity and similarity with deletions. The similarity of individuals with deletion FC-signatures were correlated (Pearson’s r) with cognitive and behavioral measures. Those included the ADOS and FSIQ in the autism sample and the PANSS in the SZ sample. The p-values associated with these correlations were corrected for multiple comparison (FDR, q < 0.05).
Similarity between 16p11.2 and 22q11.2 deletions at the regional level
We correlated the 22q11.2 group-level deletion-FC-signature with individual connectomes of 16p11.2 deletion carriers and their respective controls. We correlated as well the 16p11.2 group-level deletion-FC-signature with individual connectomes of 22q11.2 deletion carriers and their respective controls. For each region, we tested whether individuals with a deletion had significantly higher (or lower) similarity to the other deletion FC-signatures than their respective controls using a Mann-Whitney U test. We reported significant group differences after FDR correction (q < 0.05) for the number of regions (64).
Gene co-expression analyses
We used available gene expression values normalized across 34 anatomical regions of the cortex (Desikan Atlas 57), for each of the 22 and 35 genes encompassed in the 16p11.2 and 22q11.2 intervals (data available at http://neanderthal.pasteur.fr, Supplementary Table S4.1 and Material and Method).
We correlated the expression values of the genes encompassed in each CNV across the 34 brain regions to compute two separate CNV co-expression matrices (34 brain regions by genes, for each CNV). We investigated the region by region similarity of the topographical organisation of genes within both CNVs by correlating (Pearson R) the CNV co-expression profiles.
To identify genes and brain regions driving this topological similarity, we performed a PCA on the gene expression values (individuals) by regions (variables). We annotated genes with the cortical DS score 29 to correlate (Pearson R) the gene contribution to the first dimension with their cortical DS values (Supplemental Table S4.2 and Material and Method).
Supplementary Materials, Methods and Results
Supplemental Materials and Methods
Objectives and methods overview
Samples
Preprocessing
Quality Control
Gene expression preparation and analyses
Supplemental Results
Figure 1: Sensitivity analyses on age distribution in 16p11.2 deletion carriers
Figure 2: Mirror effects of gene dosage are present at the network level
Effect of Schizophrenia on FC
Effect of ASD on FC
Sensitivity analysis testing the effect of medication on FC alterations in autism
Effect of ADHD on FC
Sensitivity analysis testing the effect of sex on FC alterations in SZ and ADHD
Figure 3a: Seed regions showing significant similarity between 16p11.2 deletion and Schizophrenia
Figure 3b: Seed regions showing significant similarity between 22q11.2 deletion and Schizophrenia
Figure 3c: Seed regions showing significant similarity between 16p11.2 deletion and Autism
Figure 3d: Seed regions showing significant similarity between 22q11.2 deletion and Autism
Figure 4: Do the same seed regions contribute to the similarity between either 16p11.2 or 22q11.2 deletions and individuals with SZ and ASD?
Figure 5: Regional similarities between the individual FC profiles of subjects with a psychiatric diagnosis and FC-signatures of 16p11.2 and 22q11.2 duplications
Figure 6: Similarity between the individual FC profiles of subjects with a psychiatric diagnosis and the FC-signatures of the 16p11.2 and 22q11.2 deletions and duplications
Figure 7: Loading of 22q11.2 and 16p11.2 genes and brain regions on PC1
Figure 8: Additional information on motion for each cohort after preprocessing
Supplemental Tables
Table S1. CWAS beta estimates, ranking, region and networks labels.
Table S2. Similarity of individuals with idiopathic psychiatric disorders with deletion FC-signatures
Table S3. Association between similarity with deletion FC-signatures and symptom severity
Table S4. Gene expression values per neuroanatomical region and individual gene contribution to PCA dimensions
Funding
This research was supported by Calcul Quebec (http://www.calculquebec.ca) and Compute Canada (http://www.computecanada.ca), the Brain Canada Multi investigator research initiative (MIRI), funds from the Institute of Data Valorization (IVADO). Dr Jacquemont is a recipient of a Canada Research Chair in neurodevelopmental disorders, and a chair from the Jeanne et Jean Louis Levesque Foundation. Dr Schramm is supported by a fellowship from the Institute for Data Valorization. This work was supported by a grant from the Brain Canada Multi-Investigator initiative (Dr Jacquemont) and a grant from The Canadian Institutes of Health Research (Dr Jacquemont).
ABIDE I is supported by NIMH (K23MH087770), NIMH (R03MH096321), the Leon Levy Foundation, Joseph P. Healy, and the Stavros Niarchos Foundation.
Data in the schizophrenia dataset were accessed through the SchizConnect platform (http://schizconnect.org). As such, the investigators within SchizConnect contributed to the design and implementation of SchizConnect and/or provided data but did not participate in the data analysis or writing of this report. Funding of the SchizConnect project was provided by NIMH cooperative agreement 1U01 MH097435. SchizConnect enabled access to the following data repository: The Collaborative Informatics and Neuroimaging Suite Data Exchange tool (COINS; http://coins.mrn.org/dx). Data from one study was collected at the Mind Research Network and funded by a Center of Biomedical Research Excellence (COBRE) grant, (5P20RR021938/P20GM103472) from the NIH to Dr. Vince Calhoun. Data from two other studies were obtained from the Mind Clinical Imaging Consortium Database. The MCIC project was supported by the Department of Energy under award number DE-FG02-08ER6458. MCIC is the result of the efforts of co-investigators from the University of Iowa, University of Minnesota, University of New Mexico, and Massachusetts General Hospital. Data from another study were obtained from the Neuromorphometry by Computer Algorithm Chicago (NMorphCH) dataset (http://nunda.northwestern.edu/nunda/data/projects/NMorphCH). As such, the investigators within NMorphCH contributed to the design and implementation of NMorphCH and/or provided data but did not participate in the data analysis or writing of this report. The NMorphCH project was funded by NIMH grant RO1 MH056584.
Data from the UCLA cohort provided by Dr. Bearden (participants with 22q11.2 deletions or duplications and controls) was supported through grants from the NIH (U54EB020403), NIMH (R01MH085953, R01MH100900, R03MH105808), and the Simons Foundation (SFARI Explorer Award). Finally, data from another study were obtained through the OpenFMRI project (http://openfmri.org) from the Consortium for Neuropsychiatric Phenomics (CNP), which was supported by NIH Roadmap for Medical Research grants UL1-DE019580, RL1MH083268, RL1MH083269, RL1DA024853, RL1MH083270, RL1LM009833, PL1MH083271, and PL1NS062410.
Author contributions
C.M., S.U., S.J., and P. B., designed the overall study and drafted the manuscript.
C.M. and S.U. processed the data and performed all imaging analyses.
P.O. preprocessed the SZ data and reviewed the manuscript.
C.S. performed the statistical analyses and drafted the manuscript.
G.D. performed the gene expression analysis and built the http://neanderthal.pasteur.fr/ website.
A.L., E.D., PO, and G.H. contributed to interpretation of the data and reviewed the manuscript.
A.L. and L.K. provided the UCLA fMRI data.
A.E. contributed to interpretation of the data and reviewed the manuscript.
S.G., D.L., A.M., S.P., and E.S. provided the SZ data.
CE.B. provided the UCLA fMRI data, contributed to interpretation of the data and drafted the manuscript.
The Simons Variation in Individuals Project Consortium provided the 16p11.2 data.
All authors provided feedback on the manuscript.
Acknowledgments
References




