
Abstract
Bariatric surgery, the most effective treatment for obesity and type 2 diabetes, is associated with increased levels of the incretin hormone glucagon-like peptide-1 (GLP-1) and changes in levels of circulating bile acids. The levels of individual bile acids in the gastrointestinal (GI) tract after surgery have, however, remained largely unstudied. Using ultra-high performance liquid chromatography–mass spectrometry-based quantification, we observed an increase in an endogenous bile acid, cholic acid-7-sulfate (CA7S), in the GI tract of both mice and humans after sleeve gastrectomy. We show that CA7S is a Takeda G-protein receptor 5 (TGR5) agonist that increases Tgr5 expression and induces GLP-1 secretion. Furthermore, CA7S administration increases glucose tolerance in insulin-resistant mice in a TGR5-dependent manner. CA7S remains gut restricted, minimizing off-target effects previously observed for TGR5 agonists absorbed into the circulation. By studying changes in individual metabolites after surgery, the present study has revealed a naturally occurring TGR5 agonist that exerts systemic glucoregulatory effects while remaining confined to the gut.

This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout






Similar content being viewed by others

Data availability
All data generated or analyzed during this study are included in this article and its Supplementary information and extended data files.
Code availability
No custom code or mathematical algorithms were used in this study.
References
Batterham, R. L. & Cummings, D. E. Mechanisms of diabetes improvement following bariatric/metabolic surgery. Diabetes Care 39, 893–901 (2016).
Gloy, V. L. et al. Bariatric surgery versus non-surgical treatment for obesity: a systematic review and meta-analysis of randomised controlled trials. BMJ 347, f5934–f5934 (2013).
Abbasi, J. Unveiling the ‘magic’ of diabetes remission after weight-loss surgery. JAMA 317, 571–574 (2017).
Kaska, L., Sledzinski, T., Chomiczewska, A., Dettlaff-Pokora, A. & Swierczynski, J. Improved glucose metabolism following bariatric surgery is associated with increased circulating bile acid concentrations and remodeling of the gut microbiome. World J. Gastroenterol. 22, 8698–8719 (2016).
Fiorucci, S. & Distrutti, E. Bile acid-activated receptors, intestinal microbiota, and the treatment of metabolic disorders. Trends Mol. Med. 21, 702–714 (2015).
Ryan, K. K. et al. FXR is a molecular target for the effects of vertical sleeve gastrectomy. Nature 509, 183–188 (2014).
Patti, M.-E. et al. Serum bile acids are higher in humans with prior gastric bypass: potential contribution to improved glucose and lipid metabolism. Obesity 17, 1671–1677 (2009).
Sayin, S. I. et al. Gut microbiota regulates bile acid metabolism by reducing the levels of tauro-beta-muricholic acid, a naturally occurring FXR antagonist. Cell Metab. 17, 225–235 (2013).
Duboc, H., Taché, Y. & Hofmann, A. F. The bile acid TGR5 membrane receptor: from basic research to clinical application. Dig. Liver Dis. 46, 302–312 (2014).
Madsbad, S. The role of glucagon-like peptide-1 impairment in obesity and potential therapeutic implications. Diabetes Obes. Metab. 16, 9–21 (2014).
Khorgami, Z. et al. Trends in utilization of bariatric surgery, 2010–2014: sleeve gastrectomy dominates. Surg. Obes. Relat. Dis. 13, 774–778 (2017).
Lutz, T. A. & Bueter, M. The use of rat and mouse models in bariatric surgery experiments. Front. Nutr. 3, 25 (2016).
Alnouti, Y. Bile acid sulfation: a pathway of bile acid elimination and detoxification. Toxicol. Sci. 108, 225–246 (2009).
Sato, H. et al. Novel potent and selective bile acid derivatives as TGR5 agonists: biological screening, structure−activity relationships, and molecular modeling studies. J. Med. Chem. 51, 1831–1841 (2008).
Kawamata, Y. et al. A G protein-coupled receptor responsive to bile acids. J. Biol. Chem. 278, 9435–9440 (2003).
Maruyama, T. et al. Identification of membrane-type receptor for bile acids (M-BAR). Biochem. Biophys. Res. Commun. 298, 714–719 (2002).
Sato, H. et al. Anti-hyperglycemic activity of a TGR5 agonist isolated from Olea europaea. Biochem. Biophys. Res. Commun. 362, 793–798 (2007).
Rizzo, G. et al. Functional characterization of the semisynthetic bile acid derivative INT-767, a dual farnesoid X receptor and TGR5 agonist. Mol. Pharmacol. 78, 617–630 (2010).
Pellicciari, R. et al. Discovery of 6alpha-ethyl-23(S)-methylcholic acid (S-EMCA, INT-777) as a potent and selective agonist for the TGR5 receptor, a novel target for diabesity. J. Med. Chem. 52, 7958–7961 (2009).
Thomas, C. et al. TGR5-mediated bile acid sensing controls glucose homeostasis. Cell Metab. 10, 167–177 (2009).
Brighton, C. A. et al. Bile acids trigger GLP-1 release predominantly by accessing basolaterally located g protein-coupled bile acid receptors. Endocrinology 156, 3961–3970 (2015).
Kuhre, R. E. et al. Peptide production and secretion in GLUTag, NCI-H716, and STC-1 cells: a comparison to native L-cells. J. Mol. Endocrinol. 56, 201–211 (2016).
Kuhre, R. E. et al. Bile acids are important direct and indirect regulators of the secretion of appetite- and metabolism-regulating hormones from the gut and pancreas. Mol. Metab. 11, 84–95 (2018).
Guo, C., Chen, W.-D. & Wang, Y.-D. TGR5, not only a metabolic regulator. Front Physiol. 7, 646 (2016).
Hamilton, J. P. et al. Human cecal bile acids: concentration and spectrum. Am. J. Physiol. Gastrointest. Liver Physiol. 293, G256–G263 (2007).
Comeglio, P. et al. INT-767 prevents NASH and promotes visceral fat brown adipogenesis and mitochondrial function. J. Endocrinol. 238, 107–127 (2018).
Pathak, P. et al. Farnesoid X receptor induces Takeda G-protein receptor 5 cross-talk to regulate bile acid synthesis and hepatic metabolism. J. Biol. Chem. 292, 11055–11069 (2017).
Chen, M.-C., Chen, Y.-L., Wang, T.-W., Hsu, H.-P. & Lai, M.-D. Membrane bile acid receptor TGR5 predicts good prognosis in ampullary adenocarcinoma patients with hyperbilirubinemia. Oncol. Rep. 36, 1997–2008 (2016).
Xiong, Q. et al. Metabolite-sensing G protein coupled receptor TGR5 protects host from viral infection through amplifying type I interferon responses. Front Immunol. 9, 2289 (2018).
Eissele, R. et al. Glucagon-like peptide-1 cells in the gastrointestinal tract and pancreas of rat, pig and man. Eur. J. Clin. Invest. 22, 283–291 (1992).
Harach, T. et al. TGR5 potentiates GLP-1 secretion in response to anionic exchange resins. Sci. Rep. 2, 430 (2012).
Ferruzza, S., Rossi, C., Scarino, M. L. & Sambuy, Y. A protocol for differentiation of human intestinal Caco-2 cells in asymmetric serum-containing medium. Toxicol. Vitr. 26, 1252–1255 (2012).
Tan, H.-Y. et al. A multi-chamber microfluidic intestinal barrier model using Caco-2 cells for drug transport studies. PLoS ONE 13, e0197101 (2018).
Wilson-Pérez, H. E. et al. Vertical sleeve gastrectomy is effective in two genetic mouse models of glucagon-like peptide 1 receptor deficiency. Diabetes 62, 2380–2385 (2013).
McGavigan, A. K. et al. TGR5 contributes to glucoregulatory improvements after vertical sleeve gastrectomy in mice. Gut 66, 226–234 (2017).
Hodge, R. J. & Nunez, D. J. Therapeutic potential of Takeda-G-protein-receptor-5 (TGR5) agonists. Hope or hype? Diabetes Obes. Metab. 18, 439–443 (2016).
Cao, H. et al. Intestinally-targeted TGR5 agonists equipped with quaternary ammonium have an improved hypoglycemic effect and reduced gallbladder filling effect. Sci. Rep. 6, 28676 (2016).
Wang, S. et al. Interplay between bile acids and the gut microbiota promotes intestinal carcinogenesis. Mol. Carcinog. 58, 1155–1167 (2019).
Dawson, P. A. & Setchell, K. D. R. Will the real bile acid sulfotransferase please stand up? Identification of Sult2a8 as a major hepatic bile acid sulfonating enzyme in mice. J. Lipid Res. 58, 1033–1035 (2017).
Beuers, U., Trauner, M., Jansen, P. & Poupon, R. New paradigms in the treatment of hepatic cholestasis: from UDCA to FXR, PXR and beyond. J. Hepatol. 62, S25–S37 (2015).
Ma, K., Saha, P. K., Chan, L. & Moore, D. D. Farnesoid X receptor is essential for normal glucose homeostasis. J. Clin. Invest. 116, 1102–1109 (2006).
Schaap, F. G., Trauner, M. & Jansen, P. L. M. Bile acid receptors as targets for drug development. Nat. Rev. Gastroenterol. Hepatol. 11, 55–67 (2014).
Yao, L. et al. A selective gut bacterial bile salt hydrolase alters host metabolism. eLife 7, e37182 (2018).
Cristina, M. L., Lehy, T., Zeitoun, P. & Dufougeray, F. Fine structural classification and comparative distribution of endocrine cells in normal human large intestine. Gastroenterology 75, 20–28 (1978).
Verhoeckx, K. et al. Caco-2 cell line. Impact Food Bioact. Health 175, 103–111 (2015).
Tiscornia, G., Singer, O., Ikawa, M. & Verma, I. M. A general method for gene knockdown in mice by using lentiviral vectors expressing small interfering RNA. Proc. Natl Acad. Sci. USA 100, 1844–1848 (2003).
Blosser, W. et al. A method to assess target gene involvement in angiogenesis in vitro and in vivo using lentiviral vectors expressing shRNA. PLoS ONE 9, e96036 (2014).
Abu-Gazala, S. et al. Sleeve gastrectomy improves glycemia independent of weight loss by restoring hepatic insulin sensitivity. Diabetes 67, 1079–1085 (2018).
Acknowledgements
We thank members of the Devlin, Sheu, Clardy and Banks labs (HMS) for helpful discussions and advice. We would like to acknowledge the Blacklow and Kruse labs for help with equipment and reagents, and the BWH mouse facility. We would like to thank K. Schoonjans (Ecole polytechnique fédérale de Lausanne) for the FXR reporter plasmid. We thank the human patients who participated in the present study. This work was supported by a KL2 award from Harvard Catalyst (no. 4Kl2TR001100-04 to E.G.S.), a pilot grant from Boston Area Diabetes and Endocrinology Research Center (BADERC) (no. NIH/NIDDK P30 DK057521 to E.G.S.), an NIH MIRA grant (no. R35 GM128618 to A.S.D.), a Blavatnik Biomedical Accelerator at Harvard University grant (to A.S.D.), a Quadrangle Fund for the Advancement and Seeding of Translational Research at Harvard Medical School (Q-FASTR) grant (to A.S.D. and E.G.S.), an American Heart Association Postdoctoral Fellowship (to S.N.C.), a HMS Department of Biological Chemistry and Molecular Pharmacology Fellowship (to S.N.C), an American College of Surgeons fellowship (to D.A.H.), an NIH T32 training grant (to D.A.H. and J.N.L), and a DRC P&F program grant from the Joslin Diabetes Center (no. P30DK036836) (to A.H.V).
Author information
Authors and Affiliations
Contributions
A.S.D., E.G.S., S.N.C. and D.A.H. conceived the project and designed the experiments. S.N.C. performed the cell culture experiments, BA profiling, and transcriptional analyses and hormone quantifications on mouse tissues and blood. D.A.H. performed the mouse surgeries and the enteral administration in vivo experiments. H.A., R.S. and J.N.L. performed the gavages, OGTTs and lentiviral injection experiments. J.N.L. performed the chronic dosing experiments. M.T.H. performed NMR analyses. A.H.V. collected and provided the human samples. S.N.C., D.A.H., E.G.S. and A.S.D. wrote the manuscript. A.T. provided feedback and reviewed the manuscript. All authors edited and contributed to the critical review of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
CA7S is a subject of patents held by HMS and BWH on which S.N.C., D.A.H., E.G.S. and A.S.D. are inventors. A.S.D. is a consultant for Kintai Therapeutics and HP Hood. E.G.S. was previously on the scientific advisory board of Kitotech, Inc.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Bile acid structures.
a, Structures of bile acids in main text and figures. b, Structures of additional bile acids in Extended Data and Supplementary Information.
Extended Data Fig. 2 NMR of cholic acid-7-sulfate.
a, 1H NMR of authentic sample of cholic acid-7-sulfate (CA7S) (Cayman Chemical). b, 1H NMR of CA7S purified from the cecal contents of SG mice. Signals between 3.7 to 4.4 ppm are diagnostic of CA7S. Impurities are denoted by asterisks.
Extended Data Fig. 3 Bile acid concentrations in cecal contents of mice post-sham or post-SG.
Six weeks following surgery, cecal contents were collected from sham or SG mice after an overnight fast. Bile acids were quantified using UPLC-MS (sham, n = 12, SG, n = 15, data not marked with asterisk(s) are not significant). All bile acids with measurable concentrations above the limit of detection are shown. Tα/βMCA, tauro-alpha- and tauro-beta-muricholic acid, p = 0.53; TCA, tauro-cholic acid, p = 0.32; TγMCA, tauro-gamma-muricholic acid, p = 0.36; TωMCA, tauro-omega-muricholic acid, p = 0.68; TUDCA, tauro-ursodeoxycholic acid, p = 0.67; 7-oxo-TCDCA, 7-oxo-tauro-chenodeoxycholic acid p = 0.34; αMCA, alpha-muricholic acid, p = 0.87; βMCA, beta-muricholic acid, p = 0.59; CA, cholic acid, p = 0.28; UDCA, ursodeoxycholic acid, p = 0.85; DCA, deoxycholic acid, p = 0.48; LCA, lithocholic acid, *p = 0.02; isoLCA, isolithocholic acid *p = 0.02; 3-oxo-CA, 3-oxo-cholic acid, p = 0.08; 3-oxo-LCA, 3-oxo-lithocholic acid, p = 0.79; CDCA, chenodeoxycholic acid, *p = 0.03, two-tailed Welch’s t-test. All data are presented as mean ± SEM.
Extended Data Fig. 4 Bile acid concentrations in feces of human patients pre-SG or post-SG.
Feces were collected from patients pre-op or ~5 weeks post-op and bile acids were quantified using UPLC-MS (n = 17 patients, median 36 days after surgery, data not marked with asterisk(s) are not significant). All bile acids with measurable concentrations above the limit of detection are shown. TCDCA, tauro-chenodeoxycholic acid, p = 0.97; TDCA, tauro-deoxycholic acid, p = 0.93; CA, cholic acid, **p = 1.00×10-3; CDCA, chenodeoxycholic acid, p = 0.52; DCA, deoxycholic acid, p = 0.13; LCA, lithocholic acid, *p = 0.01; isoLCA, iso-lithocholic acid, *p = 0.03; UDCA, ursodeoxycholic acid, *p = 0.02; 3-oxo-CDCA, 3-oxo-chenodeoxycholic acid, p = 0.92; 7-oxo-CDCA, 7-oxo-chenodeoxycholic acid, p = 0.47, 3-oxo-LCA, 3-oxo-lithocholic acid, p = 0.56, two-tailed paired t-test. All data are presented as mean ± SEM.
Extended Data Fig. 5 CA7S agonizes TGR5 but not FXR, induces GLP-1 secretion, and reduces systemic glucose levels.
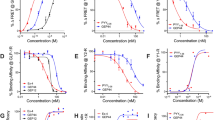
a, CA7S (500 µM) purified from SG mouse cecal contents induced secretion of GLP-1 in NCI-H716 cells compared to DMSO control (6 biological replicates per condition, **p = 1.00×10-3, two-tailed Welch’s t-test). b, Quantitative real time PCR analysis of expression of human TGR5 in TGR5 siRNA and negative (-) siRNA-treated NCI-H716 cells for Fig. 3b. c, CA7S induced an increase in intracellular calcium levels in NCI-H716 cells (4 biological replicates per condition, CA7S 10 µM *p = 0.03, 50 µM *p = 0.02, 100 µM **p = 1.80×10-3, 100 µM *p = 0.01, one-way ANOVA followed by Dunnett’s multiple comparisons test). d, CA7S induced secretion of GLP-1 in the presence of a physiologically relevant concentration of LCA (150 μM) (3 biological replicates per condition, DMSO (-) control vs. LCA **p = 9.90 × 10−3, CA7S vs. LCA 0.1 μM *p = 0.03, two-way ANOVA followed by Dunnett’s multiple comparisons test). e, CA7S did not induce activation of endogenous FXR in Caco-2 cells compared to (-) DMSO control. Known FXR agonist CDCA (10 µM) was used as a positive control (4 biological replicates per condition, CA7S 0.01-50 µM and 500–1000 µM not significant p = 0.99, CA7S 100 µM not significant p = 0.96, CDCA 10 µM **p = 4.60 × 10−3, one-way ANOVA followed by Dunnett’s multiple comparisons test). f, In vivo change in serum glucose upon acute enteral treatment with PBS and CA7S (PBS, n = 6; CA7S, n = 8 mice, ***p = 1.00 × 10−4, ns=not significant p = 0.63, two-tailed paired t-test). All data are presented as mean ± SEM.
Extended Data Fig. 6 Bile acid concentrations in cecal contents of mice treated enterally with CA7S.
Cecal contents were collected from mice after enteral treatment with CA7S or PBS and bile acids were quantified using UPLC-MS (PBS, n = 7, CA7S, n = 8, data not marked with asterisk(s) are not significant). All bile acids with measurable concentrations above the limit of detection are shown. Total BAs without CA7S, p = 0.50; Total bile acids (BAs), **p = 3.5 × 10−3; Tα/βMCA, tauro-alpha- and tauro-beta-muricholic acid, p = 0.88; TCA, tauro-cholic acid, p = 0.49; TωMCA, tauro-omega-muricholic acid, p = 0.68; 3-oxo-CDCA, 3-oxo-chenodeoxycholic acid p = 0.45; 7-oxo-CDCA, 7-oxo-chenodeoxycholic acid p = 0.87; αMCA, alpha-muricholic acid, p = 0.23; βMCA, beta-muricholic acid, p = 0.14; CA, cholic acid, p = 0.23; UDCA, ursodeoxycholic acid, p = 0.30; DCA, deoxycholic acid, p = 0.24; LCA, lithocholic acid, p = 0.50; TDCA, tauro-deoxycholic acid, p = 0.30; TCDCA, tauro-chenodeoxycholic acid, p = 0.31; CDCA, chenodeoxycholic acid, p = 0.43, two-tailed Welch’s t-test. All data are presented as mean ± SEM.
Extended Data Fig. 7 Bile acid concentrations in cecal contents of mice gavaged with one dose of CA7S.
Fasted DIO mice were gavaged with CA7S or PBS and cecal contents were collected from mice 5 hours post-gavage. Bile acids were quantified using UPLC-MS (n = 8 in each group, data not marked with asterisk(s) are not significant). All bile acids with measurable concentrations above the limit of detection are shown. Total BAs without CA7S, p = 0.35; Total bile acids (BAs), p = 0.06; Tα/βMCA, tauro-alpha- and tauro-beta-muricholic acid, p = 0.58; TγMCA, tauro-gamma-muricholic acid, p = 0.32; TCA, tauro-cholic acid, p = 0.13; TUDCA, tauro-ursodeoxycholic acid, p = 0.12; TCDCA, tauro-chenodeoxycholic acid, p = 0.13; CDCA, chenodeoxycholic acid, p = 0.33; αβMCA, alpha-muricholic acid and beta-muricholic acid, p = 0.96; CA, cholic acid, p = 0.38; TDCA, tauro-deoxycholic acid, p = 0.27; UDCA, ursodeoxycholic acid, p = 0.87; 3-oxo-CA, 3-oxo-cholic acid, p = 0.93; LCA, lithocholic acid, p = 0.86; DCA, deoxycholic acid, p = 0.76, two-tailed Welch’s t-test. All data are presented as mean ± SEM.
Extended Data Fig. 8 Bile acid concentrations in cecal contents of mice gavaged chronically with CA7S.
Cecal contents were collected from mice following an overnight fast after 48 days of daily gavage with CA7S or PBS. Bile acids were quantified using UPLC-MS (n = 7 in each group, data not marked with asterisk(s) are not significant). All bile acids with measurable concentrations above the limit of detection are shown. Total BAs without CA7S, p = 0.82; Total bile acids (BAs), p = 0.38; Tα/βMCA, tauro-alpha- and tauro-beta-muricholic acid, p = 0.46; TωMCA, tauro-omega-muricholic acid, p = 0.12; TγMCA, tauro-gamma-muricholic acid, p = 0.23; TCA, tauro-cholic acid, p = 0.09; TUDCA, tauro-ursodeoxycholic acid, p = 0.76; TCDCA, tauro-chenodeoxycholic acid, p = 0.17; αβMCA, alpha-muricholic acid and beta-muricholic acid, p = 0.23; CA, cholic acid, p = 0.06; TDCA, tauro-deoxycholic acid, p = 0.71; UDCA, ursodeoxycholic acid, *p = 0.01; CDCA, chenodeoxycholic acid, p = 0.06; DCA, deoxycholic acid, p = 0.23; LCA, lithocholic acid, *p = 0.04; 3-oxo-CA, 3-oxo-cholic acid, p = 0.30, two-tailed Welch’s t-test. All data are presented as mean ± SEM.
Supplementary information
Supplementary Information
Supplementary Tables 1 and 2, Figs. 1–14 and Note.
Rights and permissions
About this article

Cite this article
Chaudhari, S.N., Harris, D.A., Aliakbarian, H. et al. Bariatric surgery reveals a gut-restricted TGR5 agonist with anti-diabetic effects. Nat Chem Biol 17, 20–29 (2021). https://doi.org/10.1038/s41589-020-0604-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41589-020-0604-z
This article is cited by
-
Host–microbiome orchestration of the sulfated metabolome
Nature Chemical Biology (2024)
-
Research progress on the relationship between bile acid metabolism and type 2 diabetes mellitus
Diabetology & Metabolic Syndrome (2023)
-
Multilayer omics reveals the molecular mechanism of early infection of Clonorchis sinensis juvenile
Parasites & Vectors (2023)
-
Gut microbiota-mediated secondary bile acid alleviates Staphylococcus aureus-induced mastitis through the TGR5-cAMP-PKA-NF-κB/NLRP3 pathways in mice
npj Biofilms and Microbiomes (2023)
-
Glucose metabolism after bariatric surgery: implications for T2DM remission and hypoglycaemia
Nature Reviews Endocrinology (2023)
