Article Text

Abstract
Objective To determine the tolerability, safety and yield of synovial tissue in an early arthritis cohort using a minimally invasive, ultrasound (US)-guided, synovial biopsy technique in small, medium and large joints.
Methods 93 sequential biopsy procedures were assessed from a total of 57 patients (baseline and 36 repeat biopsies at 6 months) recruited as part of the ‘Pathobiology of Early Arthritis Cohort’ study. Patients completed a tolerability questionnaire prior to and following the synovial biopsy procedure. The synovial biopsy was performed under US guidance with US images of the joint recorded prior to each procedure. Synovial tissue was harvested for immunohistochemistry and RNA extraction.
Results Five different joint sites were biopsied (knee, elbow, wrist, metacarpal phalangeal and proximal interphalangeal). No significant complications were reported following the procedure. No difference in pain, swelling and stiffness of the biopsied joint from before and after the procedure was demonstrated. A median of 14 biopsy samples was retrieved from each procedure with 93% of biopsy procedures yielding good quality tissue. RNA yield was good in all joints and in repeat biopsies. Multivariant analysis demonstrated a significantly greater yield of RNA and graded tissue in relation to a high prebiopsy, grey-scale synovitis score (0–3, semiquantitative).
Conclusions A minimally invasive approach to synovial tissue harvesting, using US guidance, is both safe and well-tolerated by patients. Tissue quality/RNA yield is preserved in subsequent biopsies following therapeutic intervention. A high US grey-scale synovitis score is a predictor of good quality/quantity of tissue and RNA.
- Ultrasonography
- Synovitis
- Early Rheumatoid Arthritis
- Inflammation
Statistics from Altmetric.com
Introduction
Synovial inflammation is a key element in the pathogenesis of joint damage and disease outcome in rheumatoid arthritis (RA).1 Images studies have demonstrated that cartilage and bone damage is proportional to the level of synovitis.2 It is also known that RA synovitis is highly heterogeneous and diverse cellular and molecular signatures have been reported to be associated with different outcomes and response to therapy.3 Despite this, synovial pathobiology is not included in classification or diagnostic criteria and harvesting of synovial tissue is currently not routinely performed in clinical practice. However, synovial tissue analysis is crucial in the diagnosis of infection, malignancy and infiltrative disorders. In addition, there is great interest in retrieving synovial tissue for research purposes and proof-of-concept clinical trials where modulation of CD68-positive macrophages has been shown to correlate with effective antirheumatic therapies but not following ineffective treatment or placebo.4–7
Thus, the ability to successfully harvest good quality synovial tissue in the context of a well-tolerated and safe procedure in the hands of rheumatologists is highly desirable. Historically, synovial biopsies have been performed by a blind needle approach or conventional arthroscopy. Blind needle biopsies are well tolerated and are relatively simple to perform.8–10 Arthroscopic biopsies are technically more complicated and require theatre time but have significant advantages in being able to harvest tissue under direct visualisation. This procedure has been extensively validated with respect to tissue quality in therapeutic intervention studies, making it the accepted gold standard for synovial tissue acquisition.4 ,5 ,11–13 This has led to the emergence of relatively small number, proof-of-concept studies affording an early go/no go decision in drug development. However, arthroscopic biopsy tends to be performed in larger joints (knee and ankle), limiting recruitment of patients with suitably involved joints.
More recently, advances in ultrasound (US) imaging have facilitated the development of a minimally invasive US-guided synovial biopsy technique.14–16 This technique has been validated in a small case series using a single portal and forceps approach in nine patients with established RA.16 The authors concluded that tissue harvested from small joints using this technique represented a reliable approach for good quality tissue. There is a need to replicate these findings in a much larger cohort of patients and formally demonstrate that US-guided biopsy has an acceptable safety and tolerability profile. The ability to reliably sample synovial tissue from both large and small joints is also likely to have an impact on recruitment for early-phase therapeutic studies and broaden the usefulness of synovial biopsies as a potential tool for disease diagnosis, classification or therapeutic drug selection. Here we report the safety, tolerability, quality of synovial tissue and RNA yield in 93 consecutive minimally invasive US-guided synovial biopsies of both small, medium and large joints using an US-guided technique in early arthritis patients recruited as part of the ‘Pathobiology of Early Arthritis Cohort’ (PEAC).
Materials and methods
Patients
Fifty-seven patients were recruited as part of the PEAC (http://www.peac-mrc.mds.qmul.ac.uk) within the department of rheumatology at Barts Health NHS Trust. PEAC is a prospective multicentre study and recruits disease-modifying antirheumatic drugs (DMARDs)-naive patients with early arthritis (<1 year duration) with at least one clinically swollen joint for a baseline and 6-month follow-up synovial biopsy, along with the collection of a number of radiographic and conventional clinical parameters, including DAS28, pain and global health scores.
US evaluation and US-guided synovial biopsy technique
US examination (in grey scale and power Doppler) and US-guided synovial biopsy were performed using a General Electric (GE Healthcare, Fairfield, Connecticut, USA) Logiq 9 ultrasound machine with a two-dimensional M12L transducer—grey-scale frequency 12 MHz. Power Doppler settings were adjusted to the lowest permissible pulse repetition frequency to maximise sensitivity, and maximum colour gain was used without creating artifactual noise. Three operators (SK, FH and NN) performed all biopsies. All prebiopsy US examinations were carried out by a single ultrasonographer (MAD'A) and scored by SK and NN, blinded to the histological data. Prestudy training between the two readers was conducted with interclass correlation coefficients for synovial thickness and power Doppler reaching 0.89 and 0.98, respectively. Prebiopsy standard longitudinal US images of each biopsied joint were recorded with power Doppler switched on and off. Synovial tissue was defined as hypoechoic non-compressible intra-articular tissue exhibit or not power Doppler signal according to the OMERACT definition.17 Standard longitudinal images of individual joints prior to the US-guided procedure were viewed by an observer blinded to patient data. Synovial thickening and degree of power Doppler signal were scored using a previously reported semiquantitative score (0–3).18
The biopsy procedures were carried out in either a clean procedure room or theatre space providing sufficient expanse for an US machine, bed and sterile trolley. Each US biopsy procedure followed a similar routine with 1–3 mL of local anaesthetic injected into the soft tissues up to the joint capsule, visualised under US guidance. A further 2–5 mL of local anaesthetic (1% lignocaine) is instilled into small joints, 10–15 mL for large joints. For larger joints, a suitable coaxial outer needle may be used in addition to the Quick-Core Biopsy Needle (Cook medical, Limerick, Ireland) placed within the joint capsule—16/14G (figure 1A). A longitudinal US image is used to detect the needle and guide it to an appropriate predetermined site for biopsy. For smaller joints, a Quick-Core biopsy Needle (16G, throw length 10 mm) was used without a coaxial sheath. The maximum tolerated number of biopsies per joint was attempted with the aim for a minimum of 12 biopsies to be retrieved per procedure. Six to eight biopsies were immediately fixed in 4% paraformaldehyde for paraffin embedding and a further six immersed in 10:1 v:v of RNA-Later (Ambion) for later RNA extraction. Following the procedure, a small sterile dressing was placed over the site of the needle insertion (online video—http://www.synovialbiopsy.com). Typically, this procedure lasts 30 min from instillation of anaesthetic to final biopsy. There is little difference in the duration of procedures from small to large joints.

Histopathological scoring of synovial tissue acquired during ultrasound (US)-guided synovial biopsy. (A) Image illustrative of patient undergoing US-guided synovial biopsy of right wrist with needle placement (insert) at the scapholunate junction. (B) Representative images of synovial tissue sections ×4 magnification from US-guided synovial biopsy procedures of patients biopsied within this study cohort. 3 μm sections underwent routine staining with haematoxylin and eosin and were semiquantitatively assessed using a previously validated synovitis score 18. A composite score of 0–9 was determined following assessment of increasing lining layer thickness (A, D and G), density of the resident sublining cellular infiltrate (fibroblasts, endothelial cells and macrophages) (B, E and H) and sublining inflammatory cell infiltrate (lymphocytes and plasma cells) (C, F and I). (C) Electropherograms illustrative of RNA quality from six individual biopsy procedures (RNA integrity number).
All procedures were performed following written informed consent and were approved by the hospital’s ethics committee (REC 05/Q0703/198).
Tolerability
A standard questionnaire was administered to all patients immediately prebiopsy and postbiopsy and at their postbiopsy clinic review (3–7 days). Patients indicated pain, swelling and stiffness of the biopsied joint preprocedure and postprocedure using a visual analogue score (VAS) with tolerability being assessed using a five-point Likert scale. At their postbiopsy clinic review, patients were also asked to record how likely they were to consider a repeat biopsy in the future using a scale of highly likely, somewhat likely, unsure somewhat unlikely and highly unlikely.
Synovial histopathological assessment
From each paraffin-embedded block of synovial tissue, 3 μm thick sections obtained from three different cutting levels 50 µm apart underwent routine staining with H&E. Sections were considered valid for further histological scoring only if an intact cell lining layer was visible. A synovitis score was then assigned to each valid tissue section according to a previously described scoring system.19 Each section underwent semiquantitative assessment for three synovial membrane features: (i) thickness of the synovial lining cell layer, (ii) stroma cell density and (iii) inflammatory cell infiltrate using a scale of 0–3 (figure 1B). A composite score integrating these three features was then determined and samples categorised as no synovitis (0–1 points), low-grade synovitis (2–4 points) and high-grade synovitis (5–9 points).
RNA extraction
RNA was extracted from synovial tissue biopsies using a Trizol separation protocol. A minimum of 10 mg of synovial tissue was homogenised in cold Trizol reagent (Life Technologies, Invitrogen Division, UK). The procedure was performed using a Polytron benchtop laboratory homogeniser. Each tissue sample was kept cold (on ice) during the homogenisation procedure. Samples were processed at short 5 s intervals until all the tissue had been sheared/homogenised. Chloroform was mixed with the lysate and, following centrifugation, the aqueous RNA layer was transferred to a new microcentrifuge tube. Prechilled isopropanol was then mixed with the RNA layer. Following incubation and centrifugation, the isopropanol was removed and the RNA pellet washed with 70% ethanol. The pellet was re-dissolved in RNase-free water. The concentration/purity of the RNA sample(s) were measured using the NanoDrop 2000C (Lab Tech, UK) and the quality (RNA integrity number (RIN)) was assessed using the Agilent 2100 Bioanalyser (Agilent Technologies, UK) (figure 1C).
Statistical analyses
Demographic characteristics of patients, safety and tolerability data were described with mean (±SD) values or relative frequencies. As RNA yield was a non-parametric variable, median (IQR) or relative frequencies were used for descriptive analyses for the tissue quality data. Univariate analyses were performed using Mann–Whitney U test and Kruskal–Wallis test when appropriate. Multiple linear regressions were performed to model the percentage of graded biopsies and the quantity of RNA yield (log transformed) according to the ultrasonography score of synovial thickening (from 1 to 3), the biopsy site (small, medium or large) and the biopsy rank. p Values <0.05 were taken as statistically significant.
All statistical analyses were performed using GraphPad Prism V.3.03 (GraphPad software for Mac V.5.0).
Results
Characteristics of the study patients
Fifty-seven patients underwent baseline US evaluation and US synovial biopsy. Thirty-six of these patients were scheduled to receive a second biopsy procedure at a 6-month follow-up visit as per protocol during this period. Demographic and clinical features of patients included in the study are shown in table 1.
Summary of patient demographics and clinical characteristics of patients included in the study
US-guided synovial biopsy is a safe procedure and is well tolerated by patients
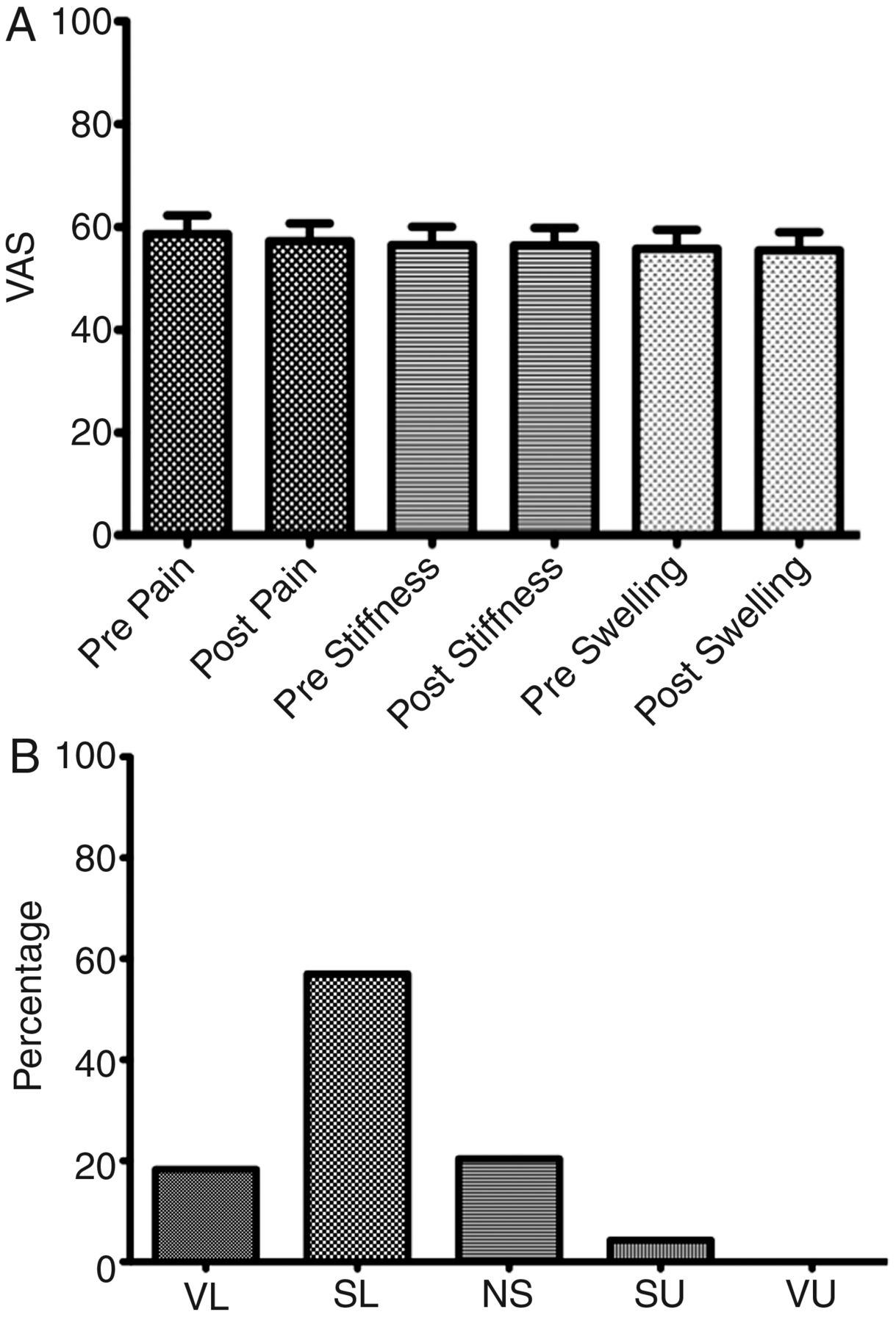
Ninety-three sequential US-guided synovial biopsy procedures are reported in this paper (57 at baseline and 36 repeat at 6 months as per PEAC protocol). Patients were asked to complete preprocedure and postprocedure VAS assessments of pain, stiffness and swelling of the biopsied joint. While there was a small trend to reduction in all postprocedure assessments, this did not reach statistical significance (figure 2A).

Ultrasound-guided synovial biopsy is a safe and well-tolerated procedure. (A) Patients were also asked to complete a visual analogue score assessing immediately prior to and following the procedure, joint pain, stiffness and swelling. No significant differences in any of the three variables preprocedure and postprocedure were reported (n=93). (B) At their postprocedure clinic visit 3–7 days following the synovial biopsy, patients were also asked to record how agreeable they were to having a subsequent synovial biopsy: very likely, somewhat likely, not sure, somewhat unlikely and very unlikely. Results are expressed as percentage of total patients (n=93).
Of the 93 US-guided procedures performed, the only reported complication was three patients feeling faint during the procedure; however, after a suitable period of time, all three patients allowed the procedure to be completed. Potential complications assessed at the postprocedure follow-up visit were infection, haemarthrosis, deep venous thrombosis, thrombophlebitis, postprocedure arthralgia and flare of the underlying disease. None of these were observed in our cohort. Notably, there were also no reported cases of wound or joint infection and no evidence of a flare of the underlying disease. The majority of patients were agreeable to having a subsequent US-guided synovial biopsy at a later date, with 81.7% of patients either ‘very likely’ or ‘somewhat likely’ to have a repeat procedure (figure 2B). In practice, 54 of the 57 patients surveyed following their first biopsy, subsequently, consented to a second biopsy (18 after locking the database for the analysis of the results presented in this paper). This represents more than 95% compliance with two US-guided synovial biopsies at baseline and at 6 months follow-up as per PEAC study protocol. At the postprocedure follow-up visit, 18 patients (19.4%) reported mild arthralgia following the procedure; however, this resolved within 24 h with simple analgesia. Patients were also asked to indicate the tolerability of the procedure using a five-point Likert scale ranging from no discomfort to severe pain (table 2). There was a significant difference in the number of patients reporting discomfort during biopsy of a large joints (elbow, knee) compared with small-sized and medium-sized joints (wrist, metacarpal phalangeal (MCP) and proximal interphalangeal (PIP)) (Fisher's exact test p=0.03). There were no significant differences between any of the other patient-reported outcomes. The safety and tolerability of US-guided biopsy is further substantiated by the fact that to date 199 patients have been recruited at Barts Health NHS Trust to the ongoing PEAC study, after locking the database for the analysis of the results presented in this paper, with 120 patients having received a second biopsy as per protocol.
Patient-reported pain/discomfort during the ultrasound-guided synovial biopsy as documented on a five-point Likert scale
US-guided synovial biopsy yields high-quality synovial tissue suitable for histopathological characterisation
Of all 93 procedures performed, 86 (92.5%) procedures yielded synovial tissue suitable for undergoing further histopathological classification for synovitis; these are subsequently referred to as ‘graded biopsies’. Biopsies were classified as high grade, low grade or uninflamed dependent on the predominant synovitis score as cited above and previously described.19 In total, 47% of procedures yielded tissue classified as low-grade synovitis and 44% high-grade synovitis, 9% of patients were classified as uninflamed. A median number of 15, 14 and 13 samples was taken respectively from small joints (MCP/PIP), medium joints (wrist) and large joints (knee and elbow).
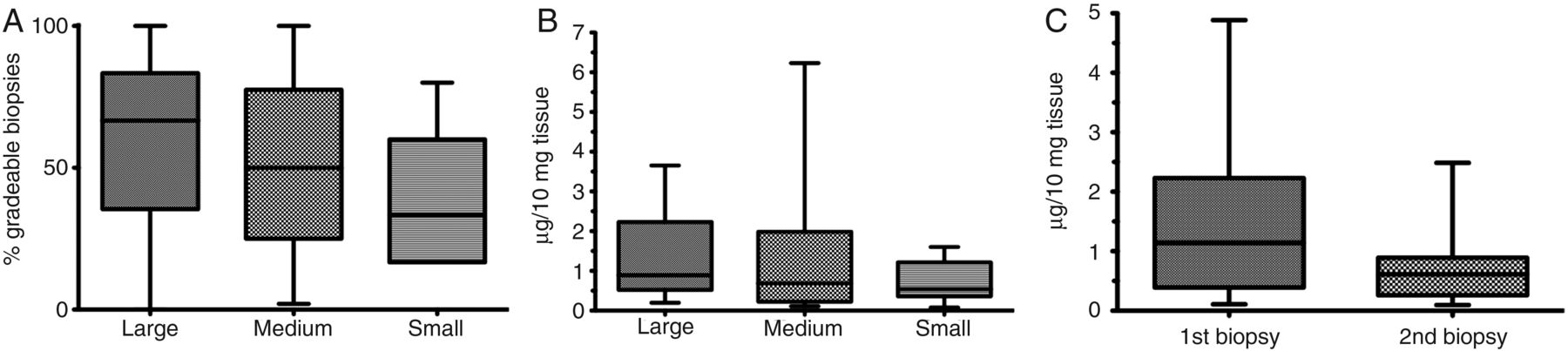
In order to determine whether yield of graded synovial tissue was dependent on size of joint, biopsied procedures were then classified into those performed on small (MCP and PIP), medium (wrist) and large (elbow and knee) joints. For each group, the mean percentage of graded tissues was reported (figure 3A). Although there was a trend for small joint biopsies to yield a fewer number of graded biopsies from individual patients, this did not reach statistical significance compared with medium and large joints.

(A) Percentage of graded synovial tissue within each biopsy procedure by joint size. (B) Total yield of RNA from biopsy samples by joint size. (C) Average total RNA yield of per biopsy procedure of first and second biopsy procedures.
US-guided synovial biopsy yields tissue sufficient for high-quality RNA extraction
The median RNA yield for each joint varied according to joint size (large: 0.89 μg/10 mg tissue; medium: 0.69 μg/10 mg tissue; small: 0.54 μg/10 mg tissue); however, no statistical difference was demonstrated between total RNA yield in each group joint size despite a tendency for smaller joints to provide a lower yield (p=0.22) (figure 3B). The average RIN was 5.32 (IQR 4.5–6.5). This demonstrates that both small and large joints can provide synovial tissue sufficient for molecular analyses.
Tissue quality and RNA yield are maintained in subsequent biopsies
A second US-guided synovial biopsy was performed in 36 patients. In all cases, US biopsy was performed on the same joint biopsied at baseline. Similar number of samples were taken at both first and second biopsies: median 14 (range 6–32) and 14 (range 4–24) samples, respectively. When the number of procedures yielding graded synovial tissue per total procedures performed following first biopsy (94.7%) and second biopsy was compared (91.6%), no significant difference was seen (p=0.70). Additionally, although total RNA yield varied from first to second biopsy, this did not reach statistical significance; first biopsy 1.14 μg/10 mg tissue (IQR 0.46–2.07) and second biopsy 0.61 μg/10 mg tissue (IQR 0.26–0.89) (p=0.08) (figure 3C), and average RIN 5.72 and 4.68, respectively.
Prebiopsy US grey-scale synovial thickness best predicts synovial tissue yields
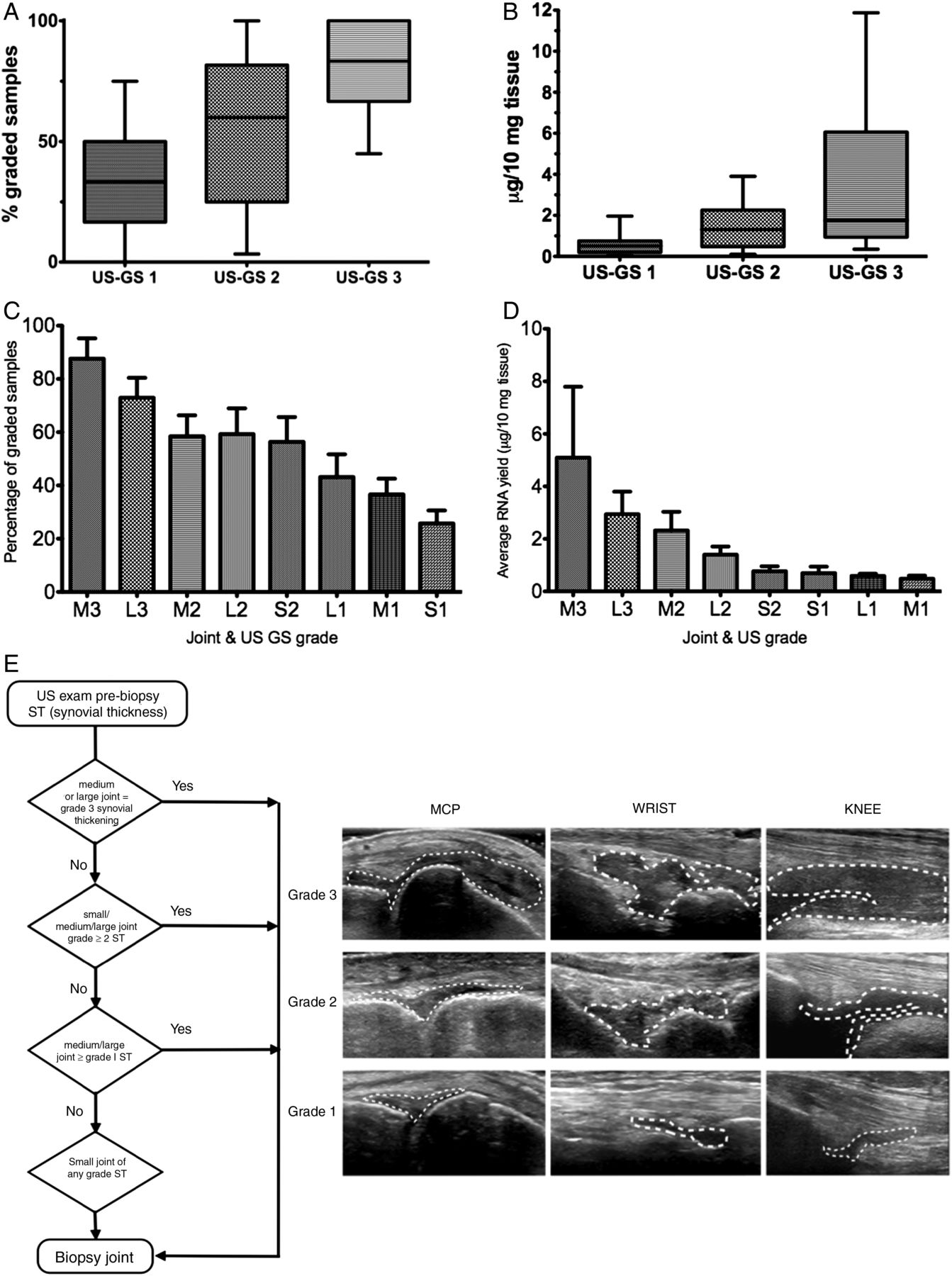
In order to determine whether prebiopsy US assessment of synovitis can predict synovial tissue quantity/quality, histological and RNA analyses were stratified according to the prebiopsy US grey-scale synovial thickness and power Doppler score (semiquantitative 0–3). As predicted, significantly higher yield of graded synovial tissue was associated with grade 3 synovial thickening versus grade 2 and grade 1 (p<0.01) (figure 4A). Similarly, significantly higher RNA yields were associated with grade 3 synovial thickening than grade 2 or grade 1 (figure 4B). Notably, no significant differences were observed when a similar analysis was performed according to prebiopsy power Doppler scores in relationship to either graded synovial tissue or RNA yield (results not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Synovial tissue quality varies with prebiopsy ultrasound (US) assessment of synovial thickening. (A) Tissue gradability by prebiopsy US grey scale (US-GS 1–3) synovial thickening assessment (Kruskal–Wallis test p<0.001). (B) Average total RNA yield by prebiopsy US grey-scale synovial thickening assessment (Kruskal–Wallis test p<0.0002). (C) Variation of graded tissue as demonstrated by joint size and US grey-scale synovial thickness score. (D) Variation of average total RNA yield as demonstrated by joint size and US grey-scale synovial thickness score. L, large joint; M, medium joint; S, small joint. US GS synovial thickness grade 1–3, for example, M2 medium joint with US grade 2 synovial thickness. (E) Suggested decision tree for guiding joint selection for US-guided synovial biopsies and metacarpal phalangeal, wrist and knee grading atlas.
Thus, using multivariant analysis and synovial thickness score, power Doppler score and joint size as variables, the degree of US-detected synovial thickening was the only independent predictor of tissue quantity/quality (figure 4C,D).
Discussion
Synovial tissue analysis has been instrumental in enhancing our understanding of RA pathogenesis and, of critical importance, the development of current targeted biological therapies.3 Thus, harvesting good quality synovial tissue is critical to further our understanding of diverse disease pathogenesis, response to therapy and developing new pharmacotherapy. To date the most convenient method of tissue collection has been at joint replacement surgery or via arthroscopic intervention. By definition, joint replacement surgery is usually performed in established/late-stage disease while arthroscopic biopsy is relatively invasive and limited to large joints, expensive and restricted to specialised centres. Thus, the ability to retrieve synovial tissue of good quality, by a safe and tolerable method, from large and small joints at the initial onset of inflammatory joint disease remains a highly desirable objective.
In this paper, we have demonstrated that a minimally invasive US-guided approach is both safe and well tolerated by patients while enabling the collection of high-quality synovial tissue.
Previous published studies describing US-guided synovial biopsies have described a portal and forceps approach retrieving 6–8 samples per joint.14–16 We have taken significantly more samples per procedure (12–15), which appears to be well tolerated by patients. To our surprise, the procedure was better tolerated in small-sized and medium-sized joints (MCP/PIP/wrists), which is likely to represent the ability to better anaesthetise smaller surface areas. PIP joints are often biopsied using a ‘ring block’ technique providing total anaesthesia to the digit. Notably, tissue quality was preserved in subsequent biopsies following therapeutic intervention as shown by the 36 patients in our cohort who received a second synovial biopsy. This is an important finding in the context of using such a technique to monitor changes in synovial biomarkers of response to therapy. While we did not demonstrate a statistical difference in terms of joint size and tissue quality, there is a suggestion that smaller joints such as MCP or PIP may yield less tissue/RNA quantity/quality. This is likely to reflect the technical difficulties in performing the biopsy at these sites. Encouragingly sufficient material for analyses could be obtained in 92.5% of patients biopsied, although within biopsies of smaller joints (MCP/PIP) the proportion of graded tissue samples fell to 40% but with sufficient RNA extracted for gene expression analysis.
US assessment prebiopsy is a useful tool for site selection and to improve tissue acquisition with joints demonstrating greater synovial thickening yielding better tissue/RNA quantity/quality. On this basis, to inform the choice of joint to be biopsied and maximise tissue yield, we developed a decision tree and an illustrative atlas shown in figure 4E.
The next issue that was addressed in this investigation was success/failure rate of the procedure. As previously mentioned, our overall success rate in obtaining good quality synovial tissue in 92.5% patients competes favourably with similar comparable US-guided biopsy procedures. For example, in the case of renal biopsies (performed routinely as part of a diagnostic work up), suitable tissue for analysis is obtained in 83–97% of case series reported.20–24 Similar results are seen in the context of liver biopsies with adequate or diagnostic liver tissue obtained in 81–97% of cases.25 In addition, major complications of renal biopsies have been quoted as between 18% and 28% in these series, while arthroscopic procedures performed by rheumatologists or orthopaedic surgeons reportedly run approximately 1% risk of a significant postprocedure complication.26 Our data also compare favourably to this, with no patients reporting a significant complication following this minimally invasive US-guided biopsy technique; however, three patients did report feeling faint during the procedure. While 93 biopsies represent the largest published cohort of patients undergoing this US-guided procedure to date, we are aware that as a developing technique safety remains an important outcome to be monitored and reported. This technique may be combined with a coaxial outer sheath allowing a single portal approach. While feasible in larger joints, a coaxial in smaller joints increases the technical difficulties, particularly in post-treatment biopsies. It would appear that repeated needling required in small joint procedures does not change the safety profile in our cohort; however, future publications should continue to report infectious, haemorrhagic and other complications that may be observed with this procedure. Importantly, this paper reports a single-centre experience and, thus, further work is needed to confirm these finding at multiple sites.
Nonetheless, this paper demonstrates that US-guided synovial biopsy is a relatively simple and rapid procedure that is safe in the hands of rheumatologists, is well tolerated by patients and enables the collection of synovial tissue from most patients and most joints (large/small). This technique will facilitate the execution of appropriately powered biopsy-driven multicentre randomised clinical trials to inform therapeutic decision making. The demonstration of clinical utility would potentially lead to the development of predictive algorithms incorporating pathobiology into existing clinical, laboratory and imaging modalities if not for all, at least for the most difficult patients. This will put the management of RA on a par level with most other medical specialties, where pathobiology constitutes an essential component in the routine management and treatment decision, including cancer27 ,28 and systemic manifestations of other rheumatic diseases such as skin, muscles, salivary glands, nerves, kidneys and blood vessels.29 ,30
References
Footnotes
-
Handling editor Tore K Kvien
-
SK and FH are joint first authors of this report.
-
Contributors All authors contributed to the conception and design of this project, were involved in the interpretation of data, drafting and revising the article and had final approval of the version to be published.
-
Funding This work was supported by a grant by the Medical Research Council to develop the Pathobiology of Early Arthritis Cohort (MRC Grant 86661).
-
Competing interests SK received a Clinical Research Fellowship from Arthritis Research UK (grant ref. 17571).
-
Ethics approval King's College Hospital Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.