Article Text

Abstract
Most intracranial haemorrhages in infants after the neonatal period are secondary to non-accidental injury. Occasionally brain haemorrhages in non-mobile infants are due to an inherited coagulopathy. This may often be diagnosed with a coagulation screen on admission. Little is known about the neurological outcome of infants in the latter group.
Five infants are described who presented with acute spontaneous brain haemorrhage secondary to an inherited coagulopathy (n = 3) and vitamin K deficiency in α1 antitrypsin deficiency (n = 1) and Alagille’s syndrome (n = 1). Despite the critical clinical presentation and the severe imaging findings, these five infants made a good neurological recovery.
Infants presenting with spontaneous ICH due to a significant (inherited) coagulopathy are usually easy to differentiate from non-accidental shaking injury; their bleeding pattern within the brain seems different from non-accidental shaking injury and neurodevelopment outcome appears better.
- infancy
- inherited coagulopathy
- intracranial haemorrhage
- outcome
- shaking
Statistics from Altmetric.com
Most intracranial haemorrhages (ICH) in infants after the neonatal period are secondary to non-accidental injury (NAI). Outcome in these children is generally poor.1–3 Occasionally brain haemorrhages in non-mobile infants are due to an inherited coagulopathy, sometimes known and sometimes diagnosed following a coagulation screen on admission. Little is known about the neurological outcome of infants in the latter group.4
Here we describe the clinical presentation, brain imaging findings, and outcome of five children with spontaneous ICH secondary to an inherited coagulopathy (n = 3), α1 antitrypsin deficiency (n = 1), and Alagille’s syndrome (n = 1). All five are from the Oxford region and presented under the age of 1; three within the past 2 years, one 4 years ago, and another 8 years ago.
CASE 1
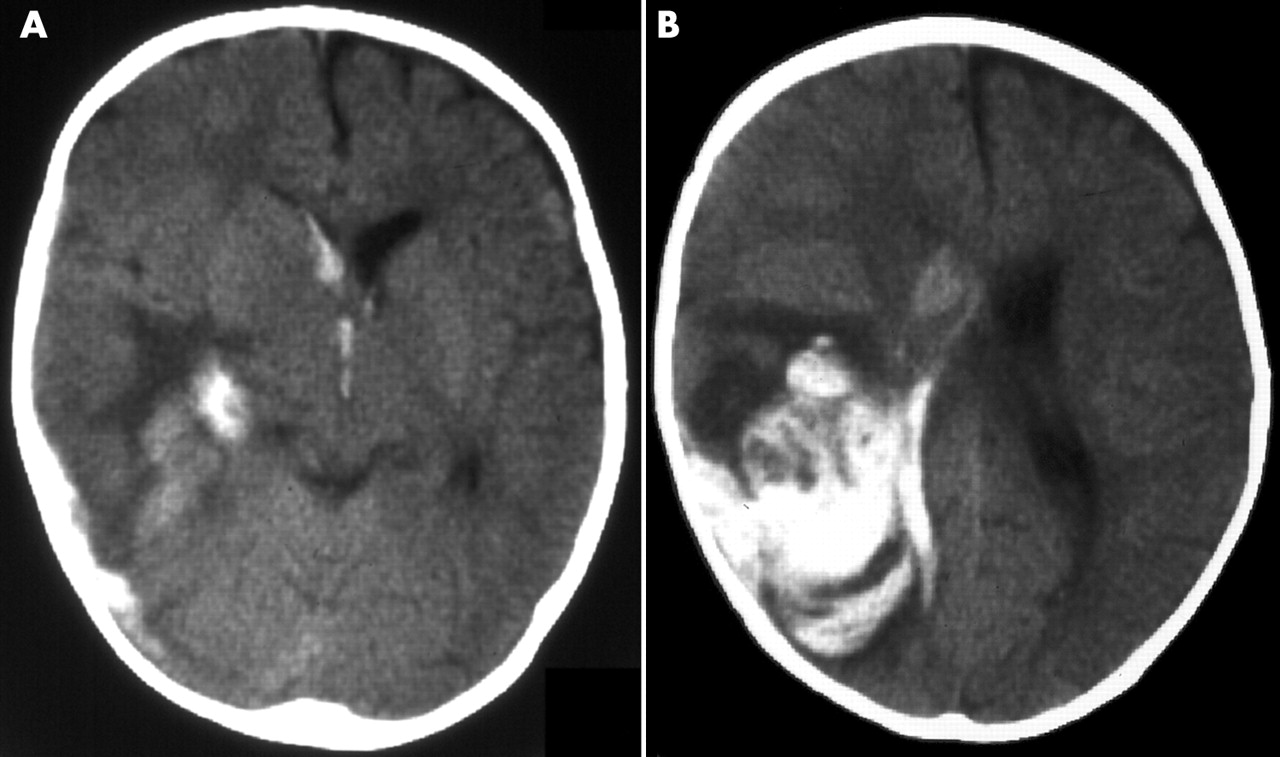
An 8 month old boy, known to have severe haemophilia A (factor VIII <1 iu/dl) but not on regular factor VIII treatment, presented with drowsiness, poor feeding, and focal seizures. On admission he appeared pale (Hb 82 g/l). Urgent computed tomography (CT) brain scan showed a right tempero-parietal haematoma with extension into the ventricular and subdural spaces (fig 1). He received factor VIII treatment and intravenous phenytoin, but was otherwise managed conservatively and did not require surgical drainage.

CT brain scan of case 1 with severe haemophilia A.
At the time of reporting he is 25 months old; his head circumference is following the 40th centile. He has developed a right hand preference but uses the left hand well. He may have a left hemianopia. The rest of his neurodevelopmental assessment is normal. Initially he had infrequent left sided seizures but he has been seizure free for over a year now and carbamazepine is gradually being withdrawn.
CASE 2
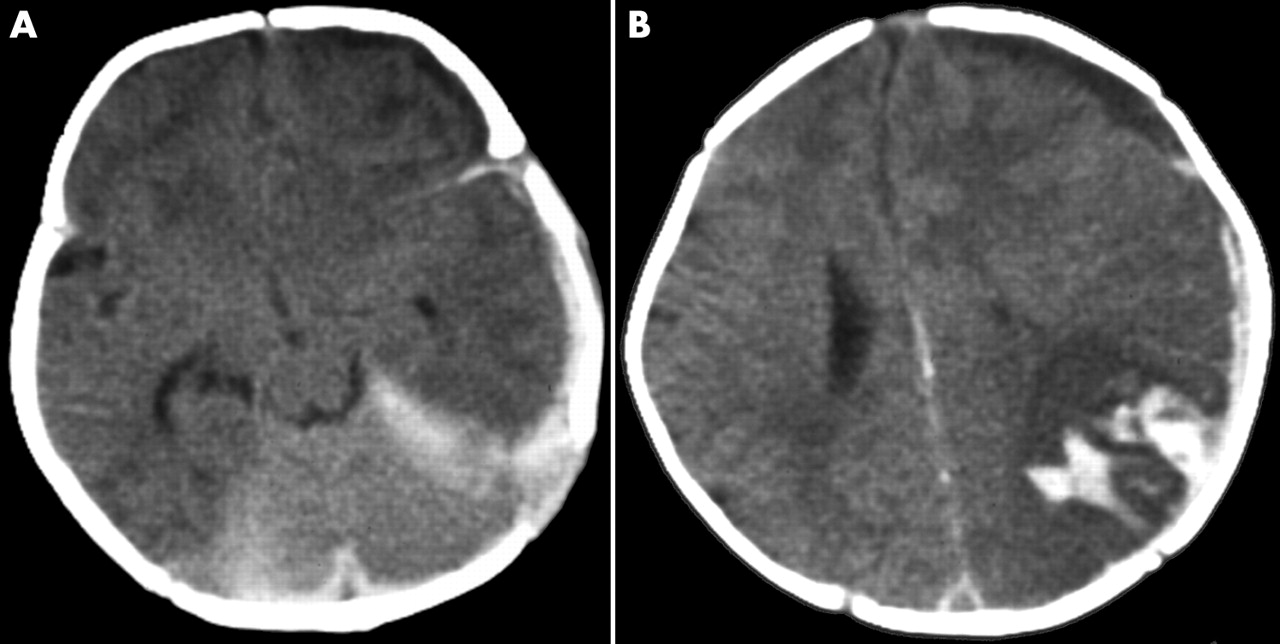
This boy received oral vitamin K at birth and was breast fed. At 6 weeks he presented with vomiting, irritability, and lethargy. He was anaemic on presentation (Hb 84 g/l), shut down, and required resuscitation including ventilatory support. His initial clotting studies were grossly abnormal (table 1), but corrected with infusions of fresh frozen plasma and intravenous vitamin K. CT brain imaging showed a left fronto-parietal haemorrhage with mass effect and left subdural blood with spread over the tentorium (fig 2).
Summary of coagulation test results of cases 1–5

CT brain scan of case 2 with a diagnosis of α1 antitrypsin deficiency.
Further investigations revealed an underlying diagnosis of α1 antitrypsin deficiency (PiZZ). He was treated with vitamin supplements, bile salts, and phenobarbitone, the latter for control of right sided seizures as well as promotion of bile flow. Phenobarbitone was discontinued four weeks after the event. He made an excellent recovery. At 2 years, he has ongoing mild raised liver transaminases and splenomegaly, but his development and neurological examination are normal.
CASE 3
This boy was born by elective caesarean section at term. On day 4 he developed seizures and vomiting. Cranial ultrasound scan showed a germinal matrix haemorrhage with intraventricular extension. Clotting studies were abnormal (table 1), leading to a diagnosis of afibrinogenaemia. He was treated with regular cryoprecipitate infusions. Cryoprecipitate treatment was discontinued at 4 months because the CT scans looked satisfactory and lack of overall consensus regarding routine ongoing fibrinogen replacement therapy.
At 9 months he returned with an acute encephalopathy and left focal seizures. He required resuscitation including mechanical ventilation. The acute CT brain scan showed a right sided parenchymal brain haemorrhage with extension to subdural and intraventricular spaces (fig 3). The prognosis at the time was thought to be very poor. Fibrinogen treatment was optimised and the clot evacuated via craniotomy. He had a postoperative left sided hemiplegia and left sided focal seizures, which gradually resolved.

{kind=link}
{kind=link}
{kind=link}
CT brain scan of case 3 with afibrinogenaemia.
Now, at over 4 years of age, his development is normal. He is bilingual and has had no further seizures. Apart from a squint, his neurological examination is normal.
CASE 4
This baby, known to have severe haemophilia A (factor VIII <1 iu/dl), presented at 11 months with vomiting, irritability, and right sided focal seizures. On assessment he was pale (Hb 73 g/l), unresponsive, and floppy. CT brain scan showed a large left posterior tempero-parietal parenchymal haemorrhage extending to the extra-axial spaces with midline shift to the right and an enlarged right ventricle. He developed brain stem compression. An emergency surgical evacuation of the clot was performed. He recovered well postoperatively.
This child is now 8 years old, attends a normal mainstream school, and has mild clumsiness only. He is right handed. He has infrequent brief right sided partial seizures and is on carbamazepine.
CASE 5
This 10 week old girl presented with irritability, reduced feeding, vomiting, and seizures. She had a tense anterior fontanelle. The acute CT brain scan showed subdural haematoma in the posterior fossa and around the tentorium. Her prothrombin time (PT) and activated partial thromboplastin time (APTT) were raised; thrombin test and fibrinogen were normal (table 1). Her haemoglobin was 65 g/l and she was found to have conjugated hyperbilirubinaemia with raised liver transaminases.
The seizures were controlled with intravenous lorazepam but she required intubation and ventilation. Her PT and APTT corrected promptly with one infusion of fresh frozen plasma and vitamin K.
Examination by the paediatric ophthalmologist excluded retinal haemorrhages. Liver ultrasound scan was normal but the liver biopsy showed a paucity of bile ducts. Chest x ray revealed a T9 butterfly vertebra and she was found to have a pulmonary branch stenosis. These findings are suggestive of Alagille’s syndrome, which was the explanation for the secondary vitamin K deficient coagulopathy. She responded well to regular vitamin supplements and ursodeoxycholic acid. She made a rapid and full recovery from the acute brain bleed. At 11 months, her neurodevelopment is progressing appropriately for age.
DISCUSSION
In our experience, absence of retinal haemorrhages and abnormal coagulation studies usually differentiates between whiplash shaking injury and coagulopathy as a cause of intracranial haemorrhage. In most infants with NAI, coagulation studies are normal on admission to hospital. A small minority of the infants with inherited coagulopathy may have a normal coagulation screen, but rare disorders such as factor XIII deficiency are readily identified by specific tests. With regard to brain imaging, it is generally accepted that subtentorial subdural haemorrhage is a highly specific feature of non-accidental shaking injury. The finding of these haemorrhages in case 5 serves to stress the importance of checking clotting studies before making a positive diagnosis of shaken baby syndrome on this isolated radiological finding.
Despite critical illness on presentation and extensive haemorrhage on brain imaging, all five infants described here have made a very good neurological recovery. In a retrospective survey of 30 children with haemophilia who presented with intracranial haemorrhage, only four had a severe neurological deficit and one died.4 This seems in contrast to what is seen in infants subjected to non-accidental whiplash shaking injury, whose neurological outcome is generally very poor.1–3
A possible explanation for a better prognosis in infants with underlying coagulopathy is that the haemorrhagic insult to the brain tends to be focal. In whiplash shaking injury, damage is more diffuse. It is suggested that in shaken baby syndrome, hyperextension/flexion injury at the cervico-medullary junction may be responsible for the occurrence of apnoea, resulting in widespread hypoxic ischaemic injury and cerebral oedema.5