Article Text

Abstract
Background Comparing rates of sudden unexpected death in infancy (SUDI) in different countries and over time is difficult, as these deaths are certified differently in different countries, and, even within the same jurisdiction, changes in this death certification process have occurred over time.
Aims To identify if International Classification of Diseases-10 (ICD-10) codes are being applied differently in different countries, and to develop a more robust tool for international comparison of these types of deaths.
Methods Usage of six ICD-10 codes, which code for the majority of SUDI, was compared for the years 2002–2010 in eight high-income countries.
Results There was a great variability in how each country codes SUDI. For example, the proportion of SUDI coded as sudden infant death syndrome (R95) ranged from 32.6% in Japan to 72.5% in Germany. The proportion of deaths coded as accidental suffocation and strangulation in bed (W75) ranged from 1.1% in Germany to 31.7% in New Zealand. Japan was the only country to consistently use the R96 code, with 44.8% of SUDI attributed to that code. The lowest, overall, SUDI rate was seen in the Netherlands (0.19/1000 live births (LB)), and the highest in New Zealand (1.00/1000 LB). SUDI accounted for one-third to half of postneonatal mortality in 2002–2010 for all of the countries except for the Netherlands.
Conclusions The proposed set of ICD-10 codes encompasses the codes used in different countries for most SUDI cases. Use of these codes will allow for better international comparisons and tracking of trends over time.
- SIDS
- Mortality
Statistics from Altmetric.com
What is already known on this topic
There are intercountry differences in International Classification of Diseases-10 (ICD-10) coding practices with regard to infant deaths that occur suddenly and unexpectedly. It has therefore been difficult to make comparisons between countries and follow trends in these deaths.
What this study adds
We propose and use a set of International Classification of Diseases-10 (ICD-10) codes that encompass the codes that could be used in different countries for sudden unexpected deaths in infancy. Utilization of this more comprehensive grouping of codes will allow for better intercountry comparisons and trends over time.
Introduction
Since sudden infant death syndrome (SIDS) was originally defined by Beckwith in 1969 as ‘the sudden death of any infant or young child which is unexpected by history, and in which a thorough postmortem examination fails to demonstrate an adequate cause of death’,1 several definitions have been proposed.2–6 Despite minor changes, the term is generally understood to refer to the sudden, unexpected death in an infant that is unexplained, even after a complete death scene investigation, thorough postmortem (autopsy) and review of the infant's clinical history. In 1965, SIDS first appeared in the International Classification of Diseases (ICD), V.8, as code 795, and subsequently as code 798.00 in ICD-9.7 ,8 ICD-10, which came into use in 1994, but was adopted for reporting mortality in subsequent years, uses the code R95 to refer to SIDS (R95.0 refers to SIDS with mention of autopsy; R95.9 to SIDS without mention of autopsy; however, in some countries, such as the USA, R95 without decimals is used).9 In both versions, any other code is given preference. ICD-10 also uses other codes, such as W75 (accidental suffocation or strangulation in bed) or R99 (other ill-defined and unspecified causes) to refer to sudden infant deaths that are unexpected and initially unexplained.9
The terms sudden unexpected death in infancy (SUDI) and sudden unexpected infant death (SUID) have recently become more widely used for deaths that occur suddenly and unexpectedly, usually in otherwise healthy infants. As most of these deaths occur during sleep or in a sleep environment, some are also beginning to refer to these deaths as sleep-related infant deaths.3 These terms are descriptive terms that are typically used at the point of presentation when the infant is unexpectedly found dead, and describe both deaths that remain unexplained and those that are subsequently explained following a death scene investigation and autopsy. The final assigned diagnosis code depends upon the findings of the death scene investigation and autopsy; however, there is great variability in investigative practices. Further, a high proportion of all SUDI do not acquire a conclusive diagnosis, even following a thorough investigation.
Furthermore, in many countries, there has been evidence of ‘diagnostic drift’ over the years because of improved protocols for death scene investigation, and as different risk factors for SIDS, such as prone positioning, are identified and then used (often inappropriately) as indicating a cause of death.10 Many countries are using terms such as ‘accidental suffocation and strangulation in bed’, ‘positional asphyxia’ and ‘unascertained’ for these sleep-related deaths. However, difficulties arise as there are no reliable pathological markers for suffocation (whether accidental or intentional), and, in most cases, it is difficult to conclusively state whether a death has been due to asphyxia. As a result, although most countries are now coding cause of infant deaths using WHO's ICD-10 codes9 or by translating local codes to ICD-10 codes (UK and Japan), there is much variability in coding. The variability in coding makes it difficult to compare rates of SIDS and SUDI across countries, and the only way to compare rates between countries has been to use total postneonatal (28–365 days)11 or 1 to 5-month mortality rates.12 However, this comparison is not entirely reliable, as postneonatal and 1 to 5-month mortality rates include all causes of death, including deaths with explained aetiology.
We, therefore, investigated the possibility of identifying all ICD-10 codes that could potentially be used for initially unexplained SUDI and then compared their use across a range of countries where such codes were used. We excluded codes that indicate a clear medical (eg, infection, metabolic disorder, arrhythmia, congenital anomaly) or forensic (eg, head injury or other trauma) cause, even if these may initially present as SUDI. Our aim was to identify if ICD-10 codes were being applied differently in different countries and to develop a more robust tool for international comparison of these types of deaths.
Methods
Eight countries (Australia, Canada, Germany, Japan, the Netherlands, New Zealand, England and Wales, USA) were identified for comparison. All were considered high-income, and there was a collaborator in each place who could provide the necessary information. All ICD-10 codes were examined independently by two authors (BJT and EAM)—both of whom are experienced clinicians and researchers in the area of postneonatal mortality—to identify an a priori list of all codes that could possibly be used when the cause of death was not clear.9 ICD-10 codes are listed in table 1, and specifically include codes that have been used when it is assumed that bed-sharing contributed to the death (eg, W75: accidental suffocation and strangulation in bed) as well as codes describing terminal events that would be secondary (ie, agonal) rather than primary causes of death under 1 year of age (eg, W78: inhalation of gastric contents; W99: inhalation and ingestion of food causing obstruction of respiratory tract).
Deaths by ICD-10 code,9 total deaths and SUDI rates (per 1000 live births), 2002–2010
Authors from each of the eight countries accessed publicly available national vital statistics data to identify the number of deaths between birth and 1 year of age with these specific ICD-10 codes for the years 2002–2010. The number and respective rates per 1000 live births (LB) were calculated with 95% CIs. Postneonatal rates were calculated as the number of deaths between 28 and 365 days of age per 1000 LB. Linear regression analysis was conducted for each country, predicting total SUDI rates over the years 2002–2010. Because this investigation used publicly available anonymous data, no ethical committee approval was required.
Results
All eight countries provided data on deaths in 2002–2010. Because there were so few deaths in the W78 and W79 categories, these data were combined. In Japan, the Ministry of Health, Labour and Welfare classify infant deaths by locally developed codes, which can be translated to ICD-10 codes. While postneonatal deaths in the UK are coded directly with ICD-10 codes, there is a different death certification process for stillbirths and neonatal deaths13 that translates main infant and maternal conditions to ICD-10 codes using an hierarchical classification system to assign nine mutually exclusive causes of death.14 Any deaths for which ICD-10 codes R95–R98 are given as a main condition in the infant are coded as sudden infant death. For the purposes of this international comparison, we included all and only those deaths coded as sudden infant death. The total number of deaths between 2002 and 2010 in these eight countries, with breakdown by ICD-10 code, is shown in table 1.
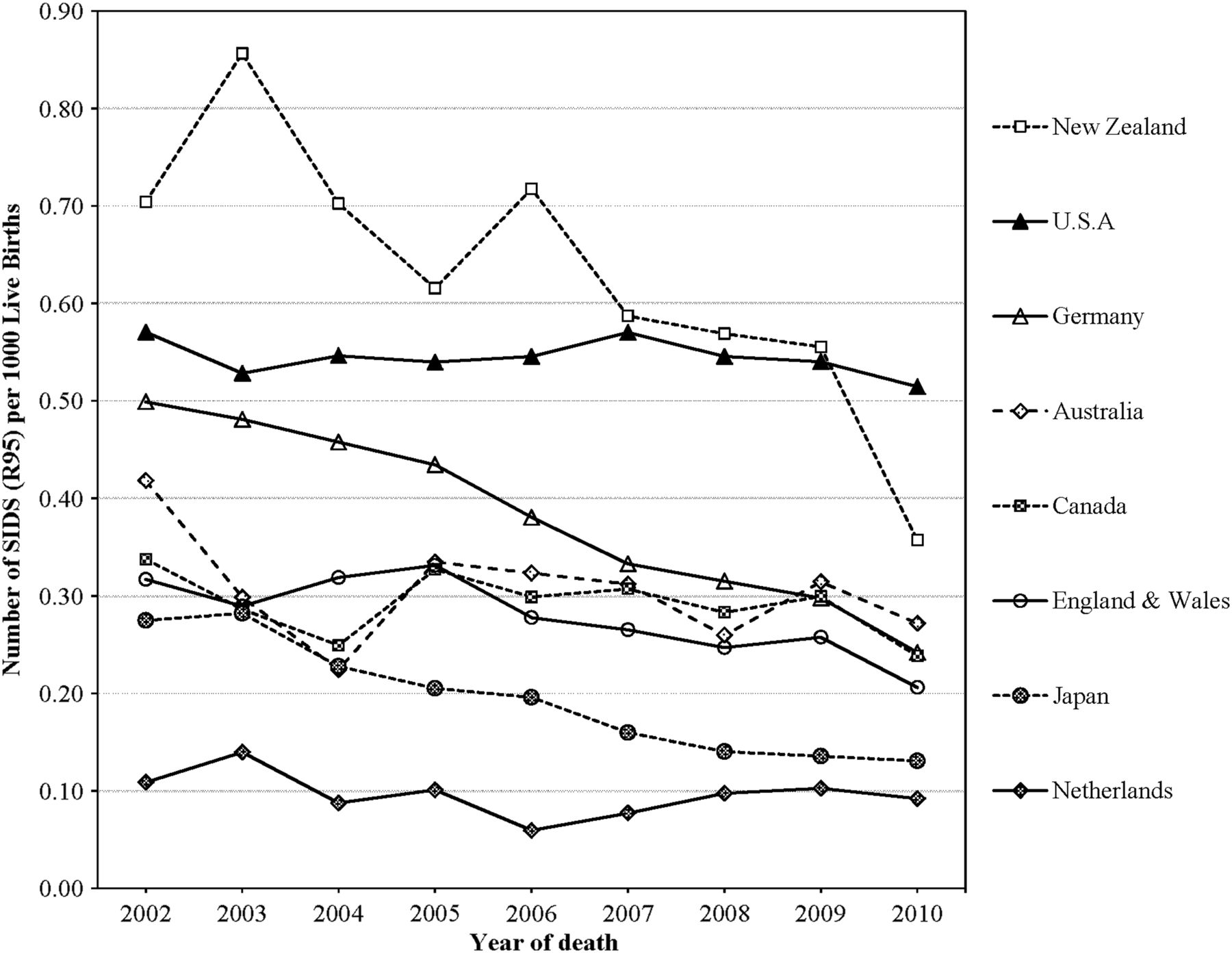
There is great variability in how each country codes SUDI (figure 1). The proportion of deaths coded as R99 (other ill-defined and unspecified causes) ranges from 3.6% in New Zealand to 36.5% in the Netherlands, and the proportion of deaths coded as W75 (accidental suffocation and strangulation in bed) ranges from 1.1% in Germany to 33.6% in New Zealand. Furthermore, Japan is the only country that consistently uses R96 (other sudden death, cause unknown) to code SUDI, with 44.8% of SUDI coded in this manner. Similarly, there is variability in the proportion of SUDI that are coded as R95 (SIDS); this ranged from 32.6% in Japan to 72.5% in Germany. Figure 2 demonstrates the rate of deaths coded as R95 in each country between 2002 and 2010.

International Classification of Diseases-10 (ICD-10) codes as percentages of the total sudden unexpected death in infancy (SUDI) per country, 2002–2010.

Rates of deaths coded as R95 (sudden infant death syndrome, SIDS), per country, 2002–2010.
Postneonatal mortality rates (per 1000 LB), as shown in table 2, range from 1.07/1000 LB in the Netherlands to 2.25/1000 LB in the USA. US A and New Zealand have higher postneonatal mortality rates than the other countries, with a less marked decline over years. Using this more comprehensive grouping of ICD-10 codes, SUDI comprises one-third to half of all postneonatal deaths for all countries except for the Netherlands (18%). The proportion of postneonatal mortality attributed to SUDI in the Netherlands is 40% lower than any of the other countries.
Postneonatal (28–365 days) mortality rates (per 1000 live births) and SUDI as a proportion of postneonatal mortality, 2000–2010
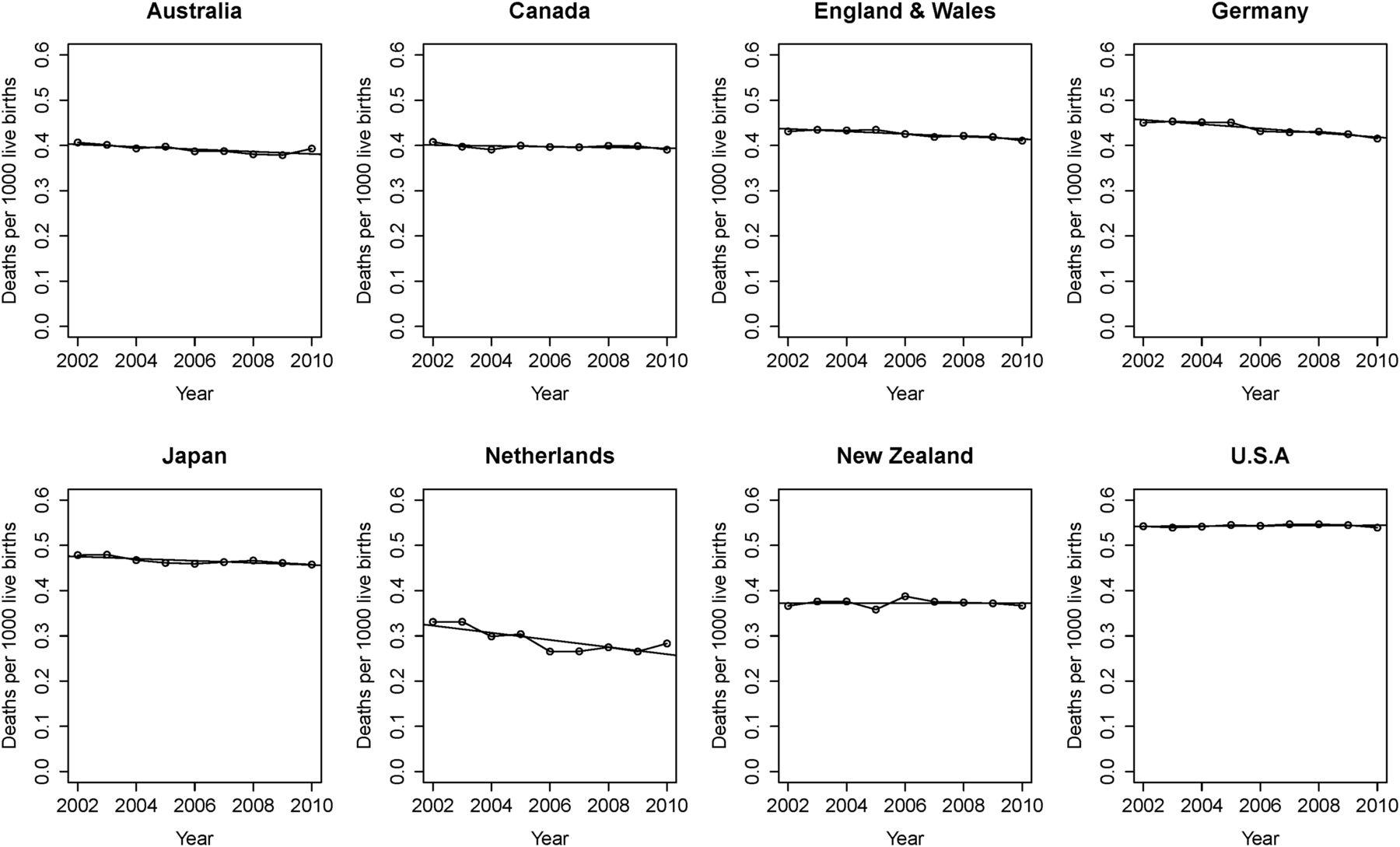
Figure 3 shows the SUDI rates (per 1000 LB) per country per year using these ICD-10 codes. The lowest overall SUDI rate is seen in the Netherlands (0.19/1000 LB), and mid-range SUDI rates (0.4–0.6/1000 LB) are seen in England and Wales (0.45/1000 LB), Canada (0.45/1000 LB), Australia (0.50/1000 LB), Germany (0.53/1000 LB) and Japan (0.60/1000 LB). The highest SUDI rates are in the USA (0.95/1000 LB) and New Zealand (1.01/1000 LB). Further, the linear trend for this period, as calculated in the linear regression analysis, is shown for each country in figure 4. All countries except the USA showed a downward pattern of total SUDI rates across the target year range, and these downward trends were statistically significant for Australia, Canada, England and Wales, Germany, Japan and the Netherlands (table 3).
Results of linear regression analysis per country of total SUDI rate, 2002–2010
Sudden unexpected death in infancy rates (per 1000 live births) per country, per year, using new set of International Classification of Diseases-10 codes.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Total sudden unexpected deaths in infancy rates per country, 2002–2010.
Discussion
Since SIDS was recognised in the 1960s, other causes of SUDI have been identified, and multiple ICD-10 codes are used variably in different countries. No code is used consistently among countries. This makes it difficult to make intercountry comparisons and to compare mortality over time. We used a more comprehensive set of ICD-10 codes that encompassed those that could be used in different countries for SUDI, and found that there was great variability in how different countries coded these deaths. Therefore, usage of this more comprehensive set of ICD-10 codes may allow for intercountry comparisons and trends over time. Further, this approach is not specific to examining and comparing rates of SUDI; this methodology could be used for any condition for which there may be inconsistent coding protocols or diagnostic drift.
When this more comprehensive set of codes is used, some interesting patterns emerge. There is great variability in the proportion of SUDI that are coded as R95 (SIDS). When SIDS rates are compared, the Netherlands and Japan have been noted to have the lowest. However, the Netherlands has the highest proportion of SUDI categorised as R99 (other ill-defined and unspecified causes of mortality), and Japan is the only country that consistently uses R96 (other sudden death, cause unknown). While other countries may rarely use this R96 code (the other seven countries in this survey collectively reported six cases in 2002–2010), Japan used this code 2655 times in this 9-year span. This suggests that different versions of diagnostic drift may be occurring, with individual countries having preference for specific ICD-10 codes.
Autopsy rates in individual countries may also impact assignment of ICD-10 codes. In the eight countries surveyed, it is estimated that autopsy rates for sudden and unexpected infant deaths ranged from <20% (Japan) to >99% (New Zealand, England and Wales). However, the comprehensiveness of the autopsy protocol may be inconsistent between countries. Further, the lack of an autopsy examination in more than 80% of SUDI in Japan may partially explain why so many deaths were coded as R96. It also suggests that Japanese codes may have lower validity, which may limit comparisons. Conversely, in other countries, when protocols for the investigation of SUDI, which include guidelines for thorough postmortem examination and complete death scene investigation, were established, rates of R95 declined, while rates of R99 and W75 increased.
When all SUDI are considered in aggregate for these eight countries (figure 3), the Netherlands continues to have the lowest rate of these deaths. Low rates of prone positioning and bed-sharing may have contributed to these low rates.15 However, Japan's SUDI rate is much higher and comparable with those in Australia, Canada, Germany and England and Wales. Unusual coding schemes such as Japan's use of R96 can have important implications beyond national boundaries. For instance, bed-sharing has been shown in many epidemiological studies to increase the risk of SIDS.16–21 Japan has been used as an exemplar of a culture in which bed-sharing is the norm, but SIDS rates are low, and many have used this as evidence that bed-sharing is a safe practice. It is likely, however, that Japan's SIDS rates are so low because most of these deaths are coded as R96 rather than R95. New Zealand and the USA stand out as having SUDI and postneonatal mortality rates consistently higher than those of other high-income countries, with little evidence of any decrease in rates. Because both the SUDI and postneonatal mortality rates in these countries are consistently high, this finding is unlikely to be explained by differences in classification, and warrants further study to determine whether there are different patterns of infant sleeping practices or other modifiable risk factors that contribute to these higher rates. Further, the variance in annual rates in New Zealand, as shown in figure 3, appears large; however, this figure does not account for the expected variance range as per 95% CIs. As New Zealand's population is much smaller than the other countries in this survey, and because New Zealand has a large number of deaths in proportion to the population, any interpretation of New Zealand's apparent rate instability should take this into account. Figure 4 sheds light on this when one compares the rates and 95% CIs for 2002 and 2010 for all countries.
We acknowledge limitations to this coding system. Usage of these eight ICD-10 codes does not resolve the issue of how different countries may code SUDI that are ultimately attributed to an infectious aetiology or to minor congenital abnormalities, and there remains great variability in how those deaths are coded. Furthermore, it is possible that this coding system does not include ICD-10 codes that may be specific to certain countries, similar to use of the R96 code in Japan. Another approach would be to use a compilation of ICD-10 codes most commonly used for postneonatal death in each of the countries; however, we specifically chose an a priori approach instead, believing that it would be less biased, particularly given the intercountry variability in coding. Further, using the most common causes of postneonatal death would likely include explained causes of death, such as infection, trauma and congenital anomalies, which were not the focus of this study. It will be important to conduct a subsequent validation study to examine which codes are most commonly used in each country to determine if additional codes are being used. Finally, these data rely on death registrations. There may be delays and inconsistencies in death registrations because of the timing and conduct of inquests. Nonetheless, these data are the most accurate internationally comparable data currently available.
In conclusion, we have proposed a more comprehensive set of ICD-10 codes that encompasses the codes that could be used in different countries for most SUDI cases, and that may better allow for intercountry comparisons and monitoring of trends over time. Such comparisons will be helpful in assessing the effectiveness of public health intervention campaigns in individual countries.
References
Footnotes
Contributors BJT conceived and designed the project, participated in the acquisition, analysis and interpretation of the data, and revised the manuscript critically for important intellectual content. JG, AE, TO, AC, JF, MV, PS and EAM participated in the acquisition and interpretation of the data, and revised the manuscript critically for important intellectual content. MH participated in analysis and interpretation of the data, and revised the manuscript critically for important intellectual content. RYM participated in the acquisition, analysis and interpretation of the data, and drafted the manuscript. All authors have approved the manuscript, and agree to be accountable for all aspects of the work.
Funding JG is currently funded by The National Institute of Health Research (NIHR) as a NIHR Doctoral Fellowship (DRF—2010-03-045).
Competing interests JG is funded by a NIHR Doctoral Fellowship to evaluate the current joint agency investigation of SUDI in England.
Provenance and peer review Not commissioned; externally peer reviewed.