Article Text

Abstract
The concept of ‘idiopathic’ Parkinson’s disease (PD) as a single entity has been challenged with the identification of several clinical subtypes, pathogenic genes and putative causative environmental agents. In addition to classic motor symptoms, non-motor manifestations (such as rapid eye movement sleep disorder, anosmia, constipation and depression) appear at prodromic/premotor stage and evolve, along with cognitive impairment and dysautonomia, as the disease progresses, often dominating the advanced stages of the disease. The key molecular pathogenic mechanisms include α-synuclein misfolding and aggregation, mitochondrial dysfunction, impairment of protein clearance (associated with deficient ubiquitin-proteasome and autophagy-lysosomal systems), neuroinflammation and oxidative stress. The involvement of dopaminergic as well as noradrenergic, glutamatergic, serotonergic and adenosine pathways provide insights into the rich and variable clinical phenomenology associated with PD and the possibility of alternative therapeutic approaches beyond traditional dopamine replacement therapies.
One of the biggest challenges in the development of potential neuroprotective therapies has been the lack of reliable and sensitive biomarkers of progression. Immunotherapies such as the use of vaccination or monoclonal antibodies directed against aggregated, toxic α-synuclein.as well as anti-aggregation or protein clearance strategies are currently investigated in clinical trials. The application of glucagon-like peptide one receptor agonists, specific PD gene target agents (such as GBA or LRRK2 modifiers) and other potential disease modifying drugs provide cautious optimism that more effective therapies are on the horizon. Emerging therapies, such as new symptomatic drugs, innovative drug delivery systems and novel surgical interventions give hope to patients with PD about their future outcomes and prognosis.
- clinical neurology
Statistics from Altmetric.com
Introduction
The clinical syndrome, described by James Parkinson in his 1817 ‘Essay on the shaking palsy’, and commonly referred to as ‘Parkinson’s disease’ (PD), is characterised by the cardinal features of rest tremor, bradykinesia, rigidity and postural instability, and a variety of other motor and non-motor symptoms.1–3 With ageing and increasing life span of the global population, age-related diseases like PD are receiving increased attention from the scientific community. Neurological disorders are now the leading source of disability in the world, and PD is the fastest growing of these disorders.4 The Global Burden of Disease Study estimates that the number of PD case will double from about 7 million in 2015 to about 13 million in 2040, suggesting a potential ‘PD Pandemic’.5 While this extrapolation based on future growth of population is just an estimate, it highlights the enormous burden that PD and related neurodegenerative conditions can pose for society.
Traditionally, the term ‘idiopathic’ PD has been used to describe the most common cause of parkinsonism in clinical practice. However, with the discovery of monogenic forms of PD (which may be clinically indistinguishable from the ‘idiopathic’ form), the clinical heterogeneity of the disease and the clinical overlap between PD dementia, dementia with Lewy bodies and other forms of parkinsonism, the nosology of PD classification needs to be continuously re-evaluated.6 7
Historic milestones
Major milestones in PD etiopathogenesis include the identification of intracytoplasmic inclusion bodies (‘Lewy bodies’) as a pathologic hallmark by Frederick Lewy in 1912 and the discovery of dopamine deficiency and its involvement in the parkinsonian animal models. The pioneering work of Arvid Carlsson and Oleh Hornykiewicz starting in 1957 established the link between dopamine deficiency and PD. The latter was supported by the proof of concept demonstrating clinical rescue in the first trial in PD patients with intravenous levodopa in 1961 and the introduction of high dosage levodopa therapy by George Cotzias in 1967.8
In 1982, William Langston, a neurologist, described seven patients in the San Francisco Bay Area who were using ‘synthetic heroin’ and developed parkinsonian features.9 Subsequent investigations revealed the cause of this drug-induced parkinsonism, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine, which is toxic to substantia nigra dopaminergic neurons. The discovery had a remarkable impact on research into the etiopathogenesis of PD and experimental therapeutics, leading to drug trials in animal models and large-scale epidemiological studies on occupational exposure to potential toxins.
In 1996, Polymeropoulos and colleagues found genetic markers on chromosome 4q21-q23 to be linked to the PD phenotype in an Italian kindred and 3 Greek families with autosomal dominant PD, and the following year they reported a mutation in the α-synuclein gene (SNCA), highlighting for the first time that PD may have a genetic aetiology.10 11 This landmark discovery launched a highly productive period of successful gene hunting during which many more PD genes and genetic risk loci were identified. These findings facilitated the generation of genetic animal models which subsequently identified new therapeutic targets for clinical trials.7 12 13
Clinical syndrome
The clinical criteria of the UK Parkinson’s Disease Society Brain Bank for probable PD require the presence of bradykinesia and one of the following features: rigidity, 4–6 Hz rest tremor, or postural instability; in addition, three supportive features are required.1 The International Parkinson’s and Movement Disorder Society (MDS) developed their own clinical diagnostic criteria that include (1) presence of parkinsonism (bradykinesia plus either rest tremor or rigidity); (2) absence of absolute exclusionary criteria, (3) supportive criteria and (4) no red flags.14 In addition to a variety of clinical rating scales, particularly the Unified Parkinson’s Disease Rating Scale (UPDRS) used to assess severity of the disease, reliable diagnostic, presymptomatic and progression biomarkers are being developed to support the diagnosis and to track the course of the disease.15
While the clinical syndrome of PD was initially attributed to basal ganglia dysfunction, human postmortem and animal model studies have subsequently shown that non-dopaminergic neurons in other brain regions (such as vagus dorsal motor nucleus, locus coeruleus and raphe nuclei) are also involved.16 These areas in the brain stem have been proposed to degenerate long before substantia nigra. Although this Braak hypothesis has been challenged,17 it is now well accepted that the involvement of non-dopaminergic pathways in the evolution of PD accounts for the increasingly recognised non-motor symptoms that adversely impact the quality of life of patients with PD.18–20 The involvement of noradrenergic, glutamatergic, serotonergic and adenosine pathways, among others, provides a biological basis for the various non-motor symptoms and suggests that modulation of these non-dopaminergic pathways can lead to alternative therapeutic approaches.21
The term ‘prodromal’ PD refers to a phase (up to 15–20 years before onset of motor symptoms) during which clinical signs of disease are not evident but underlying neurodegeneration has started and progressed22 (figure 1). Clinical studies have shown that rapid eye movement sleep behaviour disorder (RBD), depression, olfactory dysfunction, constipation and autonomic dysfunction may be present during this period.23 24 The 2019 Movement Disorders Society diagnostic criteria for prodromic PD have added other new markers (such as diabetes mellitus and physical inactivity), facilitating a web-based calculation of prodromic risk.25 The list of potential clinical, biochemical, imaging and genetic risk markers will likely continue to increase in the future.

Course of PD from prodromal phase to clinical phase, including levodopa-related complications. PD, Parkinson’s disease; PIGD, postural-instability-gait-disorder; RBD, rapid eye movement sleep behaviour disorder.
Etiology
The relative contribution of genes and environmental/lifestyle factors in pathogenesis of PD has been debated. With median age at onset at 60 years, age is the single most important risk factor for PD.26 27 The frequency appears higher in men compared with women (ratio ranges from 1.3 to 2.0) but the incidence may be influenced by differences in prevalence of variables such as cigarette smoking behaviour, use of postmenopausal hormones and caffeine intake (see section on lifestyle and protective factors).26 Like in other neurodegenerative diseases, age-related biological dysfunction including telomere dysfunction, genomic instability, epigenetic changes, ubiquitin-proteasome and autophagy-lysosomal system, and mitochondrial defects, may underpin and facilitate neuronal demise.28 29
Subtypes of PD have been proposed, categorising patients according to distinct clinical clusters, such as tremor-dominant and postural-instability-gait-disorder (PIGD) subtypes.30–33 Many studies have found that the PIGD phenotype is characterised by more severe disease manifestation and more rapid progression than the tremor-dominant for of PD. It has been suggested the clinical subtypes both determine the phenotype and natural progression/prognosis and also reflect underlying and distinct pathogenic mechanisms. This concept, however, has been challenged because motor subtypes are not fixed but change with progression of the disease and with treatment.34–36
Environmental risk factors
The potential cause and effect relationship between etiologic factors and disease has been traditionally explored through clinical association studies using a cross-sectional (hospital and community-based) or prospective (population-based) methodology. Several risk factors have been implicated including pesticide and heavy metal exposure, rural living, agricultural occupation, traumatic head injury, history of melanoma, consumption of dairy products, type 2 diabetes mellitus (reduced by the use of antidiabetic drugs), among many others26 (figure 2). Although these links are supported by underling biological plausibility, a number of the observations cannot be consistently replicated. A recent meta-analysis which involved both quantitative and qualitative analyses of various environmental exposures suggests a lack of robust consistency in some of these associations (such as rural living, well-water consumption, farming and pesticide exposure).37 While other meta-analyses reaffirmed a positive association with pesticide exposure,38 others found lack of support for a link with traumatic head injury.39 Due to several challenges and inherent limitations, it is not surprising that such epidemiological studies sometimes give conflicting results.
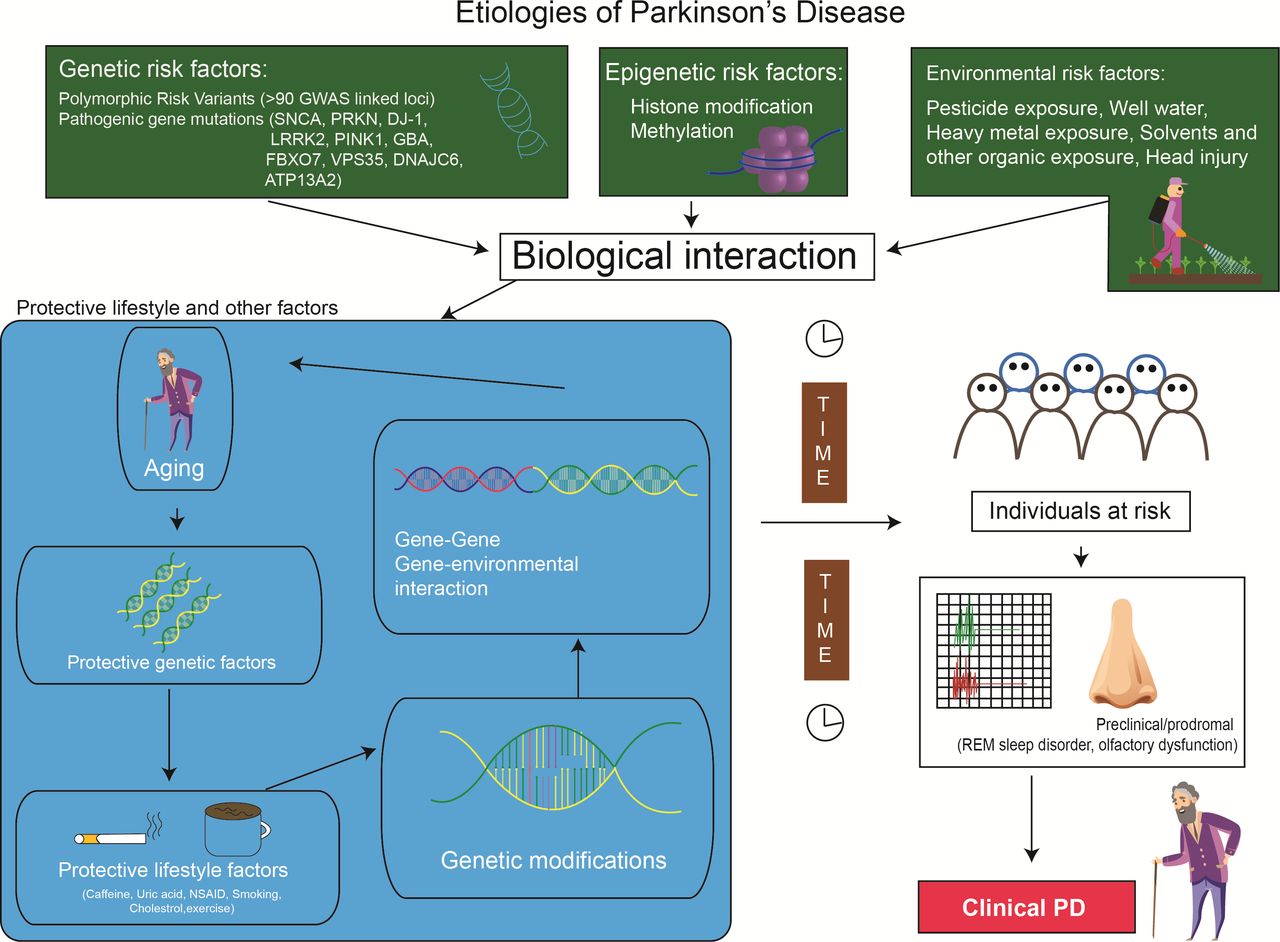
Etiologies of PD: biologic interaction between genetic, epigenetic and environmental factors. PD, Parkinson’s disease; REM, rapid eye movement.
Lifestyle and other protective factors
Cigarette smoking and caffeine consumption are the two most consistent protective factors associated with a reduced risk of PD.26 37 Other reported associations include higher serum urate, ibuprofen use and exercise, among others.26 The negative association between cigarette smoking and PD is most intriguing. This inverse relationship is not easily explained, but some have suggested that PD-related cautious personality (avoidance trait) predisposes some individuals to quitting neuroprotective smoking as the biological mechanism involved in PD.40 The other hypothesis links nicotine to dopaminergic neuronal protection since it has been shown to stimulate the release of dopamine in the striatum and preserve dopaminergic function in experimental models. It is also possible that there are other unidentified neuroprotective components in cigarette smoke.
The relative risk reduction of PD among caffeine drinkers is between 0.5 and 0.8 and, similar to smoking, a dose-dependent effect has been consistently demonstrated in most studies.26 Caffeine, an antagonist of adenosine A2a receptor, has been postulated to exert neuroprotective role by blocking this receptor. In addition to caffeine, it is possible that antioxidants present in some beverages (such as tea) may contribute to a protective effect among black tea drinkers, independent of caffeine.
Uric acid, a product of purine metabolism is an antioxidant with radical scavenger properties. A meta-analysis involving 13 studies has demonstrated that serum uric acid is lower in PD compared with controls, with the same pattern in those with more severe diseases compared with early stage PD.41 However, the Copenhagen General Population Study and some other studies have shown no causal relationship, suggesting that some unknown confounders exist.42 Ibuprofen has been suggested to lower PD risk though the association with other non-steroidal anti-inflammatory drugs has not been consistent.26 Statin use and lipid levels have also been extensively studied. However, the relative role of hydrophilic and hydrophobic statins, types of lipid levels and their specific interactions have not been conclusively addressed and methodological differences make it difficult to draw definitive conclusions.43
Genetics
Early twin studies and the identification of several families exhibiting a Mendelian inheritance pattern (dominant and recessive) provided evidence for genetic causes of PD which culminated in the discovery of the first PD-related gene, α-synuclein (SNCA), in 1997.10 A year later, mutation in Parkin (PRKN), linked to autosomal recessive form of PD, was identified.44 The nomenclature of assigning a ‘PARK’ number to these genes has been confusing and we, therefore, prefer the classification proposed by the International Parkinson and Movement Disorders Society using the gene names.6
With the advancement of genetic techniques and population studies, including genome-wide association studies (GWAS), over 20 monogenic forms of PD have been described and over 100 loci have been identified as risk factors for PD.44–47 It is daunting to decipher clinically useful information from the huge amount of published clinical and genetic data that may help differentiate the various forms of genetic parkinsonism.47 Here, we highlight some of the distinguishing features of the more important monogenetic PD disorders.
PARK-SNCA (PARK1)
Although SNCA mutations are a rare cause of PD, the pivotal role of α-synuclein in the pathogenesis of PD is now clearly recognised.16 17 48–50 A small protein, α-synuclein (140 amino acids) is involved in (1) vesicle trafficking; (2) vesicle docking and priming; (3) vesicle fusion and neurotransmitter release and (4) axonal transport, but its function in normal brain is not fully understood. Overexpression of α-synuclein in transgenic mice can cause levodopa-responsive motor impairment and nigral degeneration. The protein’s toxicity has been demonstrated with excessive amounts of wild-type (multiplication), pathogenic mutations and modification by dopamine (toxic interactions between α-synuclein oligomers and lipids). Importantly, α-synuclein (non-soluble, aggregated, fibrillar form) is a major component of Lewy bodies and Lewy neurites, the pathological hallmarks of PD. Many studies have shown that α-synuclein, pathology spreads from peripheral nervous system and olfactory bulb and then propagates from caudal brainstem rostrally (see below discussion of Braak hypothesis and staging).
Despite the rarity of SNCA mutations, the discovery of whole gene duplication, triplication and quadriplication provides considerable insights into the underlying pathogenesis involving SNCA protein and also supports earlier observations that SNCA promoter polymorphic variant increases risk in sporadic PD. SNCA triplication is associated with early onset disease (compared with duplication carriers) and cognitive impairment suggesting a gene dosage effect.
PARK-Parkin (PARK2)
Parkin (PRKN) is the most common autosomal recessive PD-related gene; compound heterozygotes for PRKN account for nearly 50% of patients with early onset PD.7 44 The disease may present with dystonic gait, leg tremor at rest and on standing, cervical dystonia, dopa-responsive dystonia. freezing, festination, retropulsion, marked sleep benefit, hyperreflexia, ataxia, peripheral neuropathy and dysautonomia. Although usually symmetrical, it may be rarely present as hemiparkinsonism-hemiatrophy. Excellent levodopa response is typically complicated by early development of levodopa-induced dyskinesia. At autopsy, there is typically loss of neurons in substantia nigra pars compacta, but the dorsal tier is well preserved and Lewy bodies are rarely present.
PARK-LRRK2 (PARK8)
LRRK2 is the most common autosomal dominant PD-related gene and a common mutation (G2019S) has been identified in both familial and sporadic PD with age-dependent penetrance.7 47 G2019S mutation accounts for 1%–3% of sporadic PD and 3%–4% familial PD in most Caucasian populations and up to 40% in North African Berbers, Iberian and Ashkenazi Jews populations.7 47 51 This mutation is largely absent in Asians who have a 5%–10% carrier rate of the ethnic specific coding risk variants (G2385R and R1628P).7 12 47 51 Most LRRK2 carriers are of late onset simulating typical PD, and clinically indistinguishable from non-carriers, but seem to have more benign course, manifested chiefly by PIGD phenotype, with less RBD and relatively preserved olfaction. Atypical features include orthostatic hypotension, dementia, hallucinations, corticobasal syndrome and primary progressive aphasia. Pathology is quite heterogeneous; it may or not include Lewy bodies and may overlap with synucleinopathies and tauopathies.
A large protein (2527 amino acids), also referred to as ‘dardarin’ (meaning tremor), LRRK2 is involved in vesicular trafficking, autophagy, protein synthesis and cytoskeletal function; it also interacts with mitochondrial proteins and may be involved in immune system. LRRK2 is highly expressed in the medium-sized spiny neurons of the striatum; also in macrophages and microglia suggesting an involvement in inflammatory pathways. Mutational hotspots are mainly in the functional domains (Kinase and Roc-Cor) suggesting a dysregulation of the kinase and GTPase activities, with a toxic gain of function as a possible underpinning mechanism.7 12
PARK-GBA
Glucocerebrosidase (GBA) gene, located on chromosome 1q21, encodes the lysosomal enzyme glucocerebrosidase that decomposes glucocerebroside into glucose and ceramide and plays an important role in sphingolipid degradation. Homozygous or compound heterozygous mutations of this gene are linked to Gaucher’s disease, the most prevalent lysosomal storage disorder. Due to low glucocerebrosidase enzymatic activity, Gaucher’s disease is associated with elevated serum chitotriosidase and glucocerebroside accumulation in the spleen, liver and bone marrow, and an increased risk of PD. Heterozygous, homozygous or compound heterozygous mutations of the GBA gene represent the single most important genetic risk factor of PD in the general population, conferring more than five times increased risk of PD.52 53 Common pathogenic variants include p.N370S, p.E326K and p.T369 M with effect sizes between 2.6 and 0.9 year reduction in age-at-onset. GBA mutations are found in 10% of sporadic PD and in over 40% of familial PD in Ashkenazi Jewish patients.54 Genetic modifiers of GBA-associated PD are being investigated in several large GWAS and other studies.55 PARK-GBA has a younger age at onset, higher prevalence of cognitive impairment and of RBD than in typical PD (in non-carriers). It has been postulated that loss-of-function of glucocerebrosidase leads to impaired lysosomal enzyme function followed by α-synuclein accumulation and aggregation. Indeed, postmortem studies of brains from PD patients with GBA mutations show Lewy bodies in cortical areas in addition to the classic PD pathology.
The rest of the pathogenic autosomal dominant (VPS35, EIF4G1, DNAJC13, CHCHD2) and autosomal recessive (PINK1, DJ1, ATP13A2, GIGYF2, PLA2G6, FBXO7, DNJAC6, SYNJ1, VPS13C) genes are quite rare and are often manifested by atypical features.3 4 40 With the easy access to direct consumer genetic testing kits and whole exome and genome sequencing services, the reported variants of uncertain significance are often difficult to interpret.56 57
Pathophysiologic mechanisms
It is well recognised in human postmortem studies that PD patients have neuronal loss in the substantia nigra par compacta, locus ceruleus and other neuronal populations.58 The Braak hypothesis suggests that the early pathological changes occur in the medulla oblongata and olfactory bulb (Braak stages 1 and 2) before advancing rostrally to substantia nigra and midbrain (Braak stages 3 and 4) by which time clinical symptoms and signs are likely to be present; in late stages, the cortical regions eventually become affected (Braak stages 5 and 6).
It is beyond the scope of this review to describe in detail the various possible pathophysiologic mechanisms. However, regardless of the underpinning etiologies (environmental, genetic or other risk factors), several key molecular events and hallmarks have been consistently reported in human postmortem tissues, in vitro human cells lines, human brain organoids and animal models (1A). These include α-synuclein misfolding and aggregation, mitochondrial dysfunction, impairment of protein clearance (involving key ubiquitin-proteasome and autophagy-lysosomal systems), neuroinflammation and oxidative stress (figure 3). These major molecular and cellular hallmarks are often associated with many other interlinked events including vesicular transport disruption, loss of microtubular integrity, neuronal excitotoxicity, disruption of trophic factors, iron metabolic pathway dysregulation, endoplasmic reticulum impairment, poly (ADP-ribose) polymerase and other enzymatic activation, among several others. Axonal mitochondria are particularly vulnerable and their dysfunction can contribute to impaired axonal transport and some have suggested that distal axons in the striatum may be the initial site of neurodegeneration in PD.59 Essentially, all of these mechanisms potentially promote programmed cell death (apoptosis) or necrosis. As cellular processes are dynamic and neurodegeneration occurs over a prolonged period of insults/stresses and with various compensatory mechanisms at play, it is impossible to determine with any certainty if these pathways work independently or converge to a single route to neuronal death. It is more likely that the various pathophysiologic processes intersect with each other, resulting in a viscous cascade of insults and ultimately irreversible cellular damage.
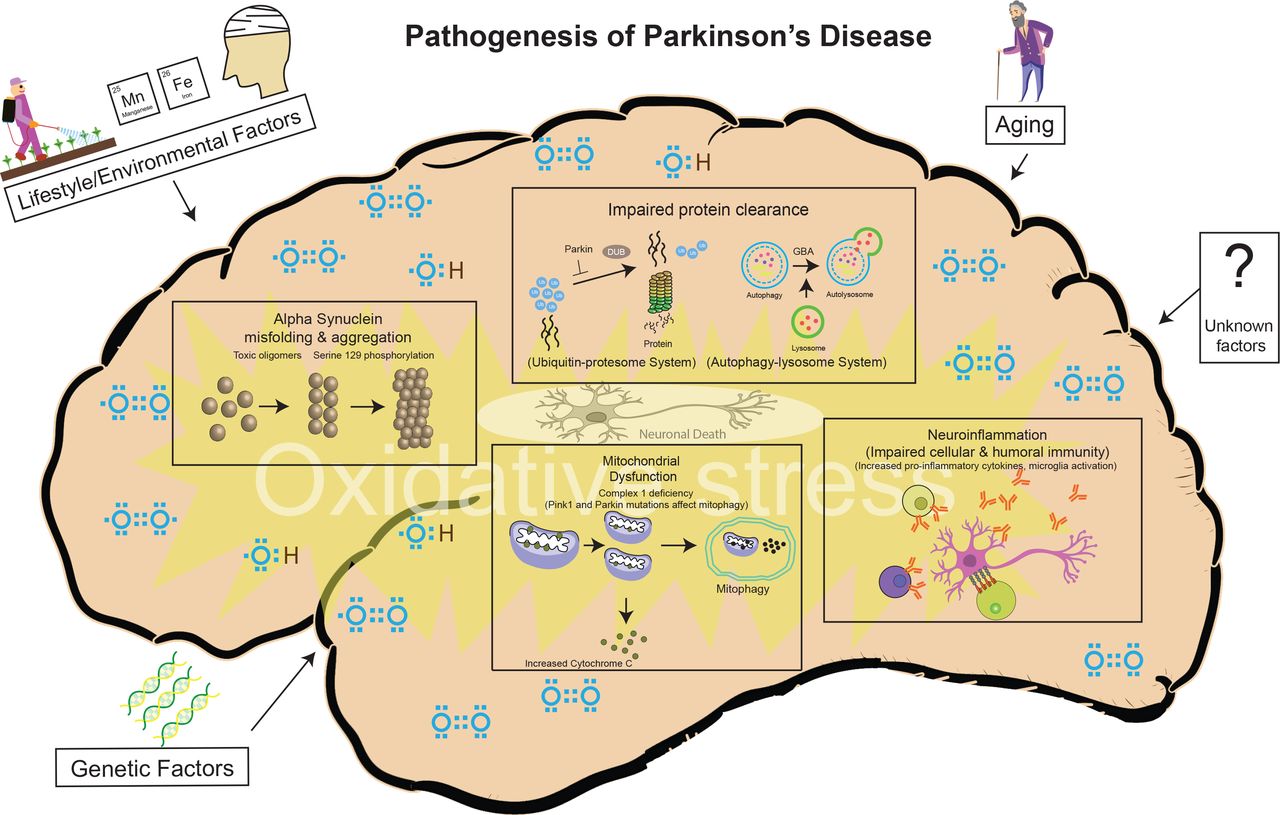
Pathogenesis of PD: a variety of cellular mechanisms on the background of oxidative stress, coupled with again, lifestyle/environmental and genetic factors contribute to the PD-related neurodegeneration. PD, Parkinson’s disease.
We highlight some of the key research pathophysiologic mechanistic insights that may have potential therapeutic implications.
α-synuclein is natively unfolded and adopts a tertiary structure on certain biochemical interactions. Abnormal aggregation of the protein has been found to be toxic to dopaminergic neurons leading to neurodegeneration associated with PD. Oxidative stress, PD gene mutations and overexpression can influence α-synuclein conformational changes and its aggregation. α-synuclein also exists in different forms/species depending on experimental conditions, and the relative toxicity of its oligomeric and fibrillar species has been debated.16 Some of these species can activate neuroinflammatory response and more importantly can ‘seed’ and spread α-synuclein pathology from cell to cell. These observations provide the basis for therapeutic approaches from inhibiting its expression to reducing oligomeric species production and cellular transmission, and some of these strategies have been translated into ongoing clinical trials.
Reduction of mitochondrial complex 1 activity has been found in PD patients and the use of its inhibitor (eg, rotenone) has been found to produce mitochondrial damage (such as decreased mitochondrial potential, with release of cytochrome c and activation of the caspase cascade and ultimate cell death) in experimental PD models. Similarly, features of mitochondrial dysfunction, including impaired mitophagy, have been identified as a result of the deleterious effects of certain PD-related gene such as Parkin, PINK1 and DJ1 (7,12,58). Investigators have also shown that mitochondrial damage promotes the accumulation of oxidised dopamine accumulation and reduced glucocerebrosidase, suggesting that dopamine is the common link between α-synuclein accumulation and lysosomal impairment.59 These studies will provide impetus for future mitochondrial targeted and antioxidant therapeutic approaches.
Both innate and adaptive immune response abnormalities have been highlighted in PD patients, including increase in proinflammatory cytokines and altered immune cell population (such as monocytes and its precursors).60 This is further supported by clinical association studies demonstrating a link between autoimmune diseases and PD, evidence of inflammatory cell activation (such as microglia) on molecular imaging and features of neuroinflammation in experimental PD models.
There is growing body of evidence of gut–brain link as a contributory factor in PD pathogenesis where vagus nerves acts as a ‘highway’ for aggregated α-synuclein to transmit from the gastrointestinal tract to the lower brainstem.61 The gut–brain interaction is supported by an experiment in which isolated from PD patients when transplanted into transgenic α-synuclein mice led to motor deficits and antibiotic treatment rescued some of the defects, and microbial recolonisation aggravated the pathophysiology. Furthermore, several studies have shown that vagotomy and appendectomy may potentially reduce the risk of developing PD. Further studies are needed to better elucidate the role of gastrointestinal microbiota and dysbiosis, infection and inflammation in triggering α-synuclein aggregation and its spread to the central nervous system as a pathogenic mechanism for PD.
Treatment
PD is a complex neurodegenerative disorder with a broad spectrum of motor and non-motor features that require individualised therapeutic approach. Clinical trials designed to provide evidence-based data must both include a well-defined population of patients and controls and should also utilise the most objective, reliable and validated tools to assess the effects of the therapeutic intervention. Although a variety of clinical rating scales and other instruments have been utilised in assessing response to various therapies, the UPDRS is used most frequently as the primary outcome measure in various clinical trials.62
An overview of medical and surgical therapeutic options for patients with PD in various stages of their disease is highlighted in table 1 and figure 4. In addition to conventional therapies, we also provide insights into evidence-based63 as well as emerging and experimental therapeutics of PD.
Drugs used in the treatment of Parkinson’s disease and levodopa-related complications

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Algorithm for the treatment of motor symptom of PD. DBS, deep brain stimulation; MAOB, imonoamine-oxidase type B inhibitor; PD, Parkinson’s disease.
Neuroprotective or disease-modifying therapies
In order to consider disease-modifying therapies, it is critical to recognise the variable slopes of progression in patients with PD, reflecting the clinical (and pathological) heterogeneity of the disease.64 An increasing understanding of etiopathogenesis of PD has led to hypotheses about potential neuroprotective strategies that, when applied early (perhaps even in the prodromal phase), may favourably alter the progression of the disease.64 However, double-blind placebo-controlled trials of potential disease-modifying therapies have been thus far disappointing64. The first such trial, DATATOP (Deprenyl and Tocopherol Antioxidative Therapy of Parkinsonism), randomised patients with early PD to treatment with selegiline (selective monoamine oxidase, MAO-B inhibitor or monoamine oxidase inhibitors (MAOI)), tocopherol (vitamin E), or both, and followed them until their disability was severe enough to require levodopa.65 Although the group randomised to selegiline had a delay in reaching the endpoint, the interpretation of the study was confounded by the drug’s mild symptomatic antiparkinsonian and antidepressant properties, as well as the potential effects of its amphetamine metabolites. Another MAOI, rasagiline, has been shown to have modest symptomatic benefit,66 but its effect on disease progression is uncertain. In a delayed-start design trial,67 used to assess the potential disease-modifying effects of rasagiline (ADAGIO (Attenuation of Disease Progression with Azilect Given Once-Daily)), 1176 patients with early untreated PD were randomised into four treatment groups: 1 or 2 mg/day, early-start vs delayed treatment). While the 1 mg dose group showed improvement in total UPDRS score and slower slope of progression compared with placebo at the end of 9 months, there was no observable benefit with the 2 mg dose. Because of the confounding symptomatic effect and lack of long-term benefits of early start rasagiline, this drug cannot be recommended as a disease-modifying treatment.
Development of neuroprotective strategies has been challenging, partly because of lack of reliable and sensitive biomarkers of progression15 and yet incomplete understanding of the pathogenesis of the disease. One of the most exciting developments of potential neuroprotective or disease-modifying therapies is the use of α-synuclein monoclonal antibodies to minimise accumulation and spread of aggregated, toxic, α-synuclein.68–70 Other antisynuclein strategies currently in development include active immunisation against synuclein, antiaggregation drugs, certain Abelson (c-Abl) kinase inhibitors, such as Nilotinib and K0706 and strategies designed to increase clearance.71 Given the history of failed ‘neuroprotective trials’, we should temper our expectations that safe and effective disease-modifying drugs will be approved in the near future.2 72
In addition, a variety of other approaches, such as the use of glucagon-like peptide 1 receptor agonists, are being explored as potential disease-modifying strategies. Furthermore, specific GBA or LRRK2 modifiers, such as ambroxol hydrochloride and DNL201 or DNL151, respectively, are currently tested in genetically defined parkinsonian populations.73 74
Symptomatic treatment of motor symptoms
Levodopa
A majority of patients with PD require levodopa therapy within 2 years of symptom onset. Levodopa, the most effective drug in the treatment of PD, is almost always combined with carbidopa or benserazide, aromatic acid decarboxylase inhibitors that prevent its peripheral metabolism and markedly reduce the risk of nausea. Increasing the ratio of carbidopa:levodopa from the current standard 1:4 has been shown to increase on time without dyskinesia and reduce off time.75
The global antiparkinsonian efficacy of levodopa is so predictable that a positive therapeutic response is used to support the diagnosis of PD. Adverse effects of levodopa include nausea and vomiting, orthostatic hypotension, sedation, confusion, sleep disturbance, hallucinations and dyskinesias. There are many different types of dyskinesia but peak-dose chorea or stereotypy and wearing off dystonia are most common.76 About half of the patients experience wearing off, and a third experience dyskinesias within 2 years after initiation of levodopa therapy. Latency from ingestion of levodopa to observable therapeutic benefit can be shortened by taking levodopa on an empty stomach (if tolerated without nausea), avoiding or reducing protein intake, or by crushing the levodopa tablet and mixing it with a carbonated beverage.
Because of a concern about development of levodopa-related motor complications, many patients and physicians are reluctant to initiate levodopa therapy even though the patients experience troublesome symptoms. This is especially true in patients with young-onset PD who are more likely to develop motor fluctuations and dyskinesia early in the course of levodopa treatment.77 78 While the treatment of PD must be individualised and tailored to the needs of each patient, this ‘levodopa phobia’ unfortunately and unnecessarily may delay needed and effective relieve of PD-related motor symptoms. Furthermore, there is no evidence from animal or human studies that levodopa accelerates disease progression or that delaying initiation of levodopa delays onset of dyskinesia. Indeed, a 9-month study, called the earlier versus later L-dopa trial, compared 150, 300 and 600 mg daily doses of levodopa with placebo found no evidence of levodopa toxicity, although 16.5% of the patients in the 600 mg group developed dyskinesia.79 Furthermore, a more recent multicenter double-blind placebo-controlled delayed-start trial using carbidopa:levodopa in early PD showed no significant change in rate of progression between early or delayed-start groups suggesting that levodopa does not have disease modifying effect.80
In patients with short duration of response to levodopa, fractionation of total daily dose is usually the initial strategy in an attempt to smooth out fluctuations and prevent wearing off symptoms (figure 4). The duration of benefit from each dose of levodopa may be enhanced by blocking dopamine metabolism with MAOIs or catechol-O-methyl transferase inhibitors (COMTIs), or by adding dopamine agonists or extended release preparations of amantadine (see below).
Different formulations of levodopa have been developed or are in development to provide more desirable delivery that avoids or prevents levodopa-related complications (table 1) 7. Studies have shown that carbidopa/levodopa extended-release (IPX066) as 95, 145, 195 and 255 mg capsules is useful in patients who continue to have motor fluctuations despite high frequency levodopa,81 though the decrease in daily ‘off’ time of about an hour is modest82 and may be comparable to other add-on oral therapies. Other formulations of levodopa that have been found effective in smoothing out motor fluctuations include continuous intrajejunal infusion of levodopa-carbidopa intestinal gel.83 The efficacy of continuous infusion formulation is comparable to subthalamic nucleus (STN) deep brain stimulation (DBS) surgery though only the latter treatment led to improvement in the duration and disability of levodopa-related dyskinesias.84 Another approach being investigated in patients with severe motor fluctuations, involves a soluble carbidopa/levodopa formulation that is continuously delivered subcutaneously via less invasive subcutaneous route that allows for a stable levodopa level over 72 hours.85 Although the preliminary data are encouraging in regard to motor fluctuations and dyskinesias, but the formation of cutaneous nodules may present a major limitation to future adaptation of this therapy.
A formulation of levodopa, approved by the US Food and Drug Administration (FDA) in 2018, as a ‘rescue’ from off periods is inhalable levodopa powder without carbidopa.86 The drug is supplied in cartons containing a 3-part inhaler and two 42 mg levodopa capsules in blister packaging. The drug must be actively inhaled and is, therefore, often associated with troublesome cough. Once patients are able to tolerate it, they can inhale it up to five times per day as needed and expect a reversal of parkinsonian symptoms within 10–30 min. The time of onset is comparable to dissolvable benserazide:levodopa formulation87 but slower than subcutaneous or sublingual apomorphine (7–10 min)88 (table 1).
Other drugs
Besides levodopa, there are many other types of medications available for the treatment of PD-related motor symptoms: anticholinergics, amantadine, MAOIs, COMTIs, dopamine agonists and istradefylline.77
Anticholinergics
Anticholinergics, such as trihexyphenidyl and benztropine, antagonise the effects of acetylcholine at muscarinic receptors postsynaptic to striatal interneurons. They are predominantly used to reduce tremor and have no effect on bradykinesia. Antagonism of acetylcholine can be associated with a variety of adverse effects such as cognitive impairment, confusion, hallucination, blurred vision, dry mouth, constipation and urinary retention. These side effects limit the usefulness of anticholinergics in the treatment of PD.
Antiglutamatergics
Glutamate mediates neurotransmission of most excitatory synapses and is vital for normal physiologic function of the brain. Amantadine (originally developed as an anti-influenza drug) is currently the main drug used in the treatment of levodopa-related dyskinesia. Besides its antiglutamatergic effect (presumably as glutamate/NMDA receptor antagonist), amantadine has also been thought to stimulate the release of endogenous dopamine stores, block reuptake of dopamine from the synaptic cleft and have anticholinergic properties. Extended release formulation of amantadine (ADS-5102 or Amantadine ER), administered before bedtime, has been found to improve both dyskinesia and also motor fluctuations. In one double-blind, placebo-controlled trial involving 126 patients, Amantadine ER significantly decreased mean off time and increased mean on time without troublesome dyskinesia.89 The most common side effects were visual hallucinations, peripheral oedema and dizziness. Amantadine ER is available as 68.5 and 137 mg capsules. Another formulation of amantadine, Osmolex ER (available as 129, 193 and 258 mg tablets), in contrast to Amantadine ER, delivers amantadine throughout the day (median Tmax 7.5 hours; half-life 16 hours). When administered in the morning, it reaches highest plasma levels during waking hours and are lowest during the night. Amantadine is contraindicated in patients with renal impairment.
Monoamine oxidase inhibitors
Although selegiline and rasagiline are most frequently used in early, mild PD, these MAOIs are also effective in patients with moderately advanced PD with levodopa-related motor complications. Another MAOI, safinamide, administered once daily (50–100 mg/day), has been found to increase mean on time without troublesome dyskinesia and reduce daily and morning off times.90 Safinamide is both a reversible MAOI and it also reduces neuronal dopamine reuptake and blocks voltage-dependent activated sodium channel and intracellular calcium entry thus reducing neuronal glutamate release.
Dopamine agonists
Dopamine receptor agonists stimulate dopamine receptors (G protein-coupled, two major families, D2-like (D1 and D5) and D1-like (D2, D3 and D4)) and when introduced early in the course of PD treatment, they delay levodopa-related complications such as motor fluctuations and dyskinesias. But evidence is lacking to support the hypothesis that early introduction of dopamine agonists slows progression of the disease or even improves long-term quality of life. Common non-ergot dopamine agonists used in clinical practice include pramipexole, ropinirole, rotigotine and apomorphine. Dopamine agonists can be used as monotherapy for motor symptoms or as an adjunct therapy when the symptoms are not sufficiently controlled by levodopa or when motor fluctuations are present.91 In an open-label randomised trial involving 1620 newly diagnosed PD patients, those who were assigned to levodopa alone reported better mobility scores compared with those on dopamine agonists or MAOBI.92 An earlier 5-year study showed that those on ropinirole has less dyskinesias compared with those on levodopa.93
The most common side effects of dopamine agonists include orthostatic hypotension, sleepiness, hallucinations and leg oedema. In addition, these drugs have been linked to relatively high frequency a variety of behavioural problems that include pathological gambling, compulsive shopping and eating, hypersexuality and other impulse-control disorders (ICD).94 Patients with PD who experience ICD seem to have a variety of associated psychiatric symptoms, such as psychosis, interpersonal sensitivity, obsessive-compulsive symptoms and depression and seem to be prone to dopamine dysregulation syndrome, an addictive behaviour associated with excessive use of dopaminergic medications.73 Patients and their care givers must be counselled about the risk of ICD before treatment initiation and at each visit, as many patients may not be forthcoming about these behaviours.95
Because of relatively high frequency of adverse effects, particularly ICD, the role of dopamine agonists has changed over the recent decades. This class of drugs is now primarily used in early treatment of PD before initiating levodopa and in patients with motor fluctuations in order to prolong the response to levodopa. In addition to two orally administered non-ergoline formulations, pramipexole and ropinirole, rotigotine is available as a patch. Apomorphine, a nonergoline dopamine agonist, is water soluble and lipophilic and is therefore suitable for intravenous, subcutaneous, sublingual, intranasal or transdermal administration.88 . Apomorphine, when administered via subcutaneous injection, may provide a rapid rescue from hypomobility end-of-dose wearing off or unpredictable on/off episodes, typically observed in advanced PD. In a study of 109 patients who were randomly assigned to receive apomorphine sublingual film or placebo, there was a significant and clinically meaningful improvement in MDS–UPDRS part 3 within 30 min, 31% of 54 patients receiving apomorphine sublingual film discontinued treatment because of oropharyngeal side effects.96 In another randomised study, apomorphine infusion (mean dose 4.68 mg/hour) reduced ‘off’ time of 2.5 hours/day compared with 0.6 hours/day with placebo in PD patients with motor fluctuations despite optimal oral or transdermal therapy.97
Catechol-O-methyl transferase inhibitors
COMTIs (entacapone, tolcapone and opicapone) block degradation of peripheral levodopa and tolcapone in addition blocks central degradation of levodopa and dopamine, increasing central levodopa and dopamine levels. Hepatotoxicity associated with tolcapone has limited its use. Triple-combination therapy containing levodopa (50, 75, 100, 125, 150 and 200 mg), carbidopa and entacapone (Stalevo) is available but often denied by third-party payers. Opicapone, a novel COMTI, administered once-daily (50 mg), has been found to significantly reduce off time.98 99 The primary role of COMTIs is to prolong the effects of levodopa and, therefore, they are useful as adjunctive drugs for patients who experience levodopa-related motor fluctuations. COMTIs are generally well tolerated, but besides increasing levodopa-related dyskinesias, they may cause nausea, postural hypotension, diarrhoea and orange discoloration of urine. There is no evidence that COMTIs prevent or delay the onset of levodopa-related motor complications.
Adenosine A2 receptor antagonist
In 2019, the FDA approved istradefylline (Nourianz), an adenosine A2 receptor antagonist, as adjunctive treatment for levodopa/carbidopa in patients with PD experiencing off episodes.100 Available as 20 and 40 mg tablets, the drug provides a modest benefit in patients with levodopa-related motor fluctuations. It is generally well tolerated, but has been reported to cause or increase dyskinesia, dizziness, constipation, nausea, hallucinations and insomnia.
Symptomatic treatment of levodopa-resistant and non-motor symptoms
Levodopa-resistant symptoms
There are many levodopa-resistant motor symptoms such as dysarthria and dysphagia, freezing of gait, postural instability and dysautonomia. Freezing, sudden immobility of the feet when attempting to walk, often associated with falls, may be seen in either the off or the on period. Although off-period freezing may improve with optimisation of medications, on-period freezing is usually resistant to pharmacologic treatment.101 102
Physical therapy, including strategies that utilise sensory cues, such as stepping over a horizontal laser beam, may be helpful.103 Dysarthria and dysphagia are often treated by speech and voice therapists. Injection of botulinum toxin has been found to be effective in controlling high-amplitude rest and postural hand tremor which may be resistant to levodopa.104 Botulinum toxin may be also beneficial in the treatment of a variety of other non-levodopa responsive parkinsonian symptoms such as blepharospasm, apraxia of eyelid opening, anterocollis, camptocormia, bruxism, sialorrhea, seborrhea, hyperhidrosis, overactive bladder and constipation.105
Non-motor symptoms
It is well recognised that non-motor symptoms comprise an important component of the clinical spectrum of PD even though most of them present with motor symptoms initially. These non-motor symptoms include depression, anxiety, apathy, psychosis, impulse control dysfunction, cognitive impairment, dementia, autonomic dysfunction (drooling orthostatic hypotension, urinary retention/incontinence, erectile dysfunction, gastrointestinal dysfunction excessive sweating), insomnia, RBD, olfactory dysfunction, pain and fatigue.106 Non-motor symptoms can affect quality of life, even more than motor problems. RBD, olfactory dysfunction and gastrointestinal dysfunction may precede motor symptoms. The Movement Disorders Society study group conducted a detailed review of available therapies for non-motor symptoms in PD.106
Here we highlight treatment of some of the common non-motor symptoms. Donepezil and rivastigmine (cholinesterase inhibitors) and memantine (NMDA receptor antagonist) provide modest benefit in patients with PD-associated dementia. Hallucinations, often associated with PD dementia and/or triggered by anti-PD drugs, usually improve with atypical antipsychotics such as quetiapine and clozapine which, in contrast to other antipsychotics (dopamine receptor blockers), have a relatively low risk of exacerbating parkinsonism. Pimavanserin, a non-dopaminergic and selective serotonin inverse agonist with high affinity at the 5-HT2A receptor, has been approved by the FDA in 2016 for the treatment of hallucinations and delusions associated with PD.107 It is available as a 10 mg tablet or 34 mg capsule.
Cholinesterase inhibitors, in addition to improving cognitive function, may reduce hallucinations, improve postural stability and might even reduce the frequency of falls in some patients.108 Sleep disorders should be addressed by strategies designed to improving sleep hygiene, and if needed, supplemented by hypnosedatives, tricyclic antidepressants, mirtazapine, trazodone, quetiapine or nighttime dopaminergic therapy.109 Excessive daytime sleepiness may respond to methylphenidate, modafinil or armodafinil.
Treatment of dysautonomia associated with PD is beyond the scope of this article but readers are referred to an excellent review of this topic.110 Orthostatic hypotension can be managed conservatively with salt supplementation, fludrocortisone, midodrine and droxidopa. Urological medications, such as migrabegron, and botulinum toxin injections into the bladder wall may improve bladder dysfunction. Dietary changes along with medications such as linaclotide and lubiprostone may improve constipation.111
Finally, the important role of physical, occupational and speech/voice therapy coupled with regular exercise programme cannot be overemphasised.112 The effectiveness of home-based and remotely supervised aerobic exercise in reducing the off-state MDS–UPDRS score was demonstrated in a double-blind, randomised clinical trial.113 One meta analysis of eight prospective studies with 2192 PD patients with a mean follow-up of 12 years demonstrated that high or moderate (but not light) physical activity reduced the risk of PD, with the association stronger in men than women.114 The PD risk reduction was between 10% and 17% for every each 10 metabolic equivalent of task-hours/week increase in high or moderate physical activity.
Surgical treatment
Deep brain stimulation
Despite optimal medical therapy, many patients with moderate to advanced disease have a poor quality of life because of fluctuating response, troublesome dyskinesia or levodopa-unresponsive symptoms. Ablative surgical approaches such as stereotactic destruction of physiologically defined overactive brain nuclei (thalamotomy, pallidotomy) have been largely replaced by DBS using implanted pulse generators. The chief advantage of DBS over ablative lesioning is that the stimulation parameters can be customised to the needs of the patient in order to optimise the benefits. Thalamic DBS is most frequently used to control high-amplitude tremor in patients with essential tremor, but STN or globus pallidus interna (GPi) are the most frequent targets for DBS treatment of patients with PD with disabling tremor and/or levodopa-related motor complications. To address the question whether optimal medical therapy or DBS provides more robust improvement, 255 patients at seven Veterans Affairs and six university hospitals were enrolled in a randomised controlled trial designed to compare the effects of DBS (STN, n=60; or GPi, n=61) and ‘best medical therapy’ (n=134) after 6 months of treatment.115 Patients treated with DBS gained a mean of 4.6 hours/day of on time without troubling dyskinesia, compared with 0 hours/day for patients who received best medical therapy (p<0.001). Furthermore, motor function improved by five or more points on the motor UPDRS in 71% of DBS and 32% of medical therapy patients. This was accompanied by improvements in the majority of PD-related health-related quality of life measures and only minimal decrement in neurocognitive testing. The overall risk of experiencing a serious adverse event, however, was 3.8 times higher in the DBS than in the medical therapy group (40% vs 11%).
The relative efficacy of STN and GPi as therapeutic targets has been debated since the advent of DBS.3 The Veterans Affairs Cooperative Study investigated STN and GPi DBS outcomes after 24 months in 299 patients, and there were no differences in mean changes in the motor (part III) UPDRS between the two targets.116 Patients undergoing STN required a lower dose of DAs than those undergoing pallidal stimulation (p=0.02), and visuomotor processing speed declined more after STN than after GPi stimulation (p=0.03). On the other hand, there was worsening of depression after STN DBS, but mood improved after GPi DBS (p=0.02). Slightly more than half of the patients experienced serious adverse events, but there was no difference in the frequency of these events between the two groups. Based on these and other studies, there is emerging evidence that GPi DBS may be particularly suitable for patients who may have troublesome dyskinesias as well as mild cognitive or behavioural impairment, whereas bilateral STN DBS may be the surgical choice for patients who are cognitively intact but in whom reduction in levodopa dosage is the primary goal. Compared with GPi, STN DBS seems to have a greater beneficial impact on off periods but is more likely associated with adverse effects such as ICD.
One common clinical question is whether DBS surgery at an earlier stage of PD or at a younger age can lead to similar positive outcome.3 In a randomised trial involving 251 relatively young (mean age 52 years) PD with early motor complications, STN DBS plus medical therapy was compared with medical therapy alone. The quality of life scores mean score improved by 7.8 points in DBS group compared with 0.2 point worsening in medical group. Motor disability, activities of daily living, levodopa-related motor complications were better in the surgery group.117 When considering early DBS, it is important to first optimise medical treatment, including strategies to improve motor fluctuations and dyskinesia and to consider the risks of surgery and other factors.118 119
While DBS is a proven effective therapeutic strategy, its success depends on the appropriate selection of patients and the experience and skill of the stereotactic surgeon in order to optimise the results and minimise complications. Advances in DBS technology, such as the use of adaptive stimulation, improving connectivity, directional stimulation and an exploration of for new targets will likely continue to improve.120 121
Focused ultrasound
Unilateral focused ultrasound lesioning of the STN or thalamus (in tremor-dominant forms of PD) has been found to be beneficial in some patients, particularly if the symptoms are markedly asymmetric.89 Finally, spinal cord stimulation is increasingly being explored in patients with PD who are most troubled by their gait disorder.122
Cell replacement therapies
The outcomes of prior fetal tissue-derived cell transplants in PD have been variable. Although some transplanted patients showed some initial improvement, many developed ‘off’ dyskinesias despite robust graft survival.123 The presence of troubling dyskinesias in some patients, ethical concerns and the restricted availability of the tissues limited the clinical applicability of fetal transplantation.
Advances in the generation dopaminergic neurons from somatic human cells and improvement in the efficacy of differentiation protocols have led to a resurgence of cell transplantation in PD.124–127 Human embryonic stem cell lines and somatic cells which can be converted into authentic midbrain dopaminergic cells that satisfy good manufacturing practice grade criteria can be generated in unlimited amounts for clinical application.124–127
In 2020 a single case report of a patient with PD who was implanted with induced pleuripotent stem cells derived from his own fibrobalsts has generated controversy because of questionable scientific and ethical issues.127 Separately, a clinical trial involving 12 PD patients was conducted in Australia using parthenogenetic stem cells (derived from chemically induced unfertilized oocytes).128 There has been no report of any adverse side effects. The trial has been completed and results are expected in first half of 2020. The TRANSEURO is an open-label multicentre European study using human fetal dopamine cells and will be completed in 2021.129 Eleven patients have received transplantation in this observational study that recruited younger early PD. Although stem cell-derived cells have advantages over fetal cells, including near-unlimited availability, several critical issues, including potential tumorigenicity, immunosuppressive therapies, off-target effects, techniques of surgical delivery devices must be addressed before these approaches become clinically available.130
Finally, surgical delivery of gene therapy is an emerging area of experimental therapeutics. In phase 1 study, 15 patients with moderately advanced PD underwent MRI-guided delivery of adeno-associated viral vector serotype-2 encoding the complementary DNA for the enzyme, aromatic L-amino acid decarboxylase (VY-AADC01) into the putamen.131 This resulted in up to 42% coverage of the putamen and up to 79% corresponding increases in enzyme activity assessed by PET. There were dose-related improvements in clinical outcomes, including increases in patient-reported ON-time without troublesome dyskinesia and quality of life at 12 months. A phase 2 trial, randomised, placebo surgery controlled, double-blinded, multicentre, phase 2 clinical trial, evaluating the efficacy and safety of VY-AADC02 in advanced Parkinson’s disease patients with motor fluctuations, is currently being conducted in multiple centres.
In conclusion, much progress has been made in the understanding the etiopathogenesis of PD and in the symptomatic treatment of PD-related symptoms. However, currently there are no effective neuroprotective or disease modifying therapies that would slow the progression of the disease. The physical, mental, social and economic burden of PD is daunting and continues to be the most challenging therapeutic hurdle, especially in the advanced stages of the disease.
Acknowledgments
Dr Jankovic has received research/training funding from AbbVie; Acadia Pharmaceuticals; Allergan; Biotek; Cerevel Therapeutics; CHDI Foundation; Dystonia Coalition; Emalex Biosciences; F. Hoffmann-La Roche Ltd; Huntington Study Group; Medtronic Neuromodulation; Merz Pharmaceuticals; Michael J Fox Foundation for Parkinson Research; National Institutes of Health; Neuraly; Neurocrine Biosciences; Parkinson’s Foundation; Parkinson Study Group; Prilenia Therapeutics; Revance Therapeutics; Teva Pharmaceutical Industries Ltd. Dr Jankovic has served as consultant/advisory board for Aeon BioPharma; Nuvelution Pharma; Teva Pharmaceutical Industries Ltd, on the editorial boards of Expert Review of Neurotherapeutics; Journal of Parkinson’s Disease; Medlink; Neurology in Clinical Practice; The Botulinum Journal; PeerJ; Therapeutic Advances in Neurological Disorders; Toxins; Tremor and Other Hyperkinetic Movements; Toxins; UpToDate; and has received royalties from Cambridge; Elsevier; Medlink: Neurology; Lippincott Williams and Wilkins; Wiley-Blackwell. Dr Tan is supported by the National Medical Research Council (STaR & PD-LCG-002 SPARK II).
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 67.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
Footnotes
Contributors JJ and EKT drafted the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.
Data availability statement No data are available. No data are available as this is a review.