Article Text

Abstract
Objective Diffuse iron deposition in the brain is commonly found in older people. One of the possible mechanisms that contribute to this iron deposition is cerebral small vessel disease. The aim of this study is to quantify diffuse iron deposition in patients with the hereditary small vessel disease cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL).
Methods 25 NOTCH3 mutation carriers and 18 healthy controls were examined using high-resolution T2*-weighted imaging on a 7 T whole body MRI scanner. Susceptibility-weighted MRI scans were analysed for areas of signal loss and increased phase shift. Phase shift measurements in deep grey nuclei, cortex and subcortical white matter were compared between mutation carriers and controls. For confirmation, ex vivo brain specimens from another three patients with CADASIL were analysed for iron deposition using ex vivo MRI combined with iron histochemistry.
Results In vivo MRI showed areas of decreased signal intensity and increased phase shift in mutation carriers. Compared with healthy controls, mutation carriers had significantly higher phase shift in the putamen (p=0.0002) and caudate nucleus (p=0.006). Ex vivo MRI showed decreased signal intensity in the putamen and caudate nucleus in all specimens. Histochemistry confirmed the presence of iron deposition in these nuclei.
Conclusions This study demonstrates increased diffuse iron accumulation in the putamen and caudate nucleus in patients with the small vessel disease CADASIL. This supports the hypothesis that small vessel disease contributes to the process of increased iron accumulation in the general population.
- CADASIL
- MRI
- iron deposition
- basal ganglia
- Alzheimer's disease
- headache
- genetics
Statistics from Altmetric.com
Introduction
Signs of increased iron deposition in the brain are frequently found on MRI scans of older people.1 This has often been considered a normal finding in healthy ageing. However, over the last few years, evidence is increasing that iron deposition is an important biomarker of various disease processes in the brain, including neurodegenerative and vascular diseases.2 ,3 It is possible that disease processes that go clinically unnoticed, such as early Alzheimer's disease or subclinical cerebral small vessel disease, contribute to iron deposition in older people.
In the general population it is hard to study the independent effect of these disease processes on iron deposition. Alzheimer's disease and cerebral small vessel disease are hard to diagnose with certainty during life, and in studies where a diagnosis has been made, confounding effects of the possible concomitant other disease processes remained a major limiting factor.2 ,3
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a hereditary small vessel disease caused by mutations in the NOTCH3 gene.4 The mutations cause abnormalities in small calibre arteries and arterioles of the cerebrum, consisting of deposition of granular osmiophilic material, degeneration of vascular smooth muscle cells and fibrous thickening of the vessel wall.5 The resulting MRI abnormalities and clinical characteristics share many similarities with sporadic small vessel disease in older people. Because of these well established vascular changes in CADASIL, and because of the relatively young age of the patients in whom concomitant Alzheimer's disease is unlikely to play a role, CADASIL is an interesting model disease to study the effect of small vessel disease on iron deposition in the brain.
The aim of this study is to investigate the potential presence and pattern of iron accumulation in the small vessel disease CADASIL, using high-field MRI in vivo and ex vivo, and histopathological confirmation of iron accumulation.
Methods
Patients
Participants consisted of 25 symptomatic (n=14) or asymptomatic (n=11) NOTCH3 mutation carriers (MCs) and 18 healthy age-matched and sex-matched volunteers recruited by an advertisement. Informed consent was obtained from all participants. Approval for the study was given by the medical ethics committee of the Leiden University Medical Center.
A full medical history was obtained. Disease duration was determined based on first occurrence of neurological symptoms excluding migraine aura.
In vivo MRI
MRI was performed on a whole body human 7 T MR system (Philips Healthcare, Best, the Netherlands), equipped with a quadrature transmit and 16-channel receive head coil (Nova Medical, Wilmington, Massachusetts, USA). Whole brain imaging was performed with all sequences in an axial plane parallel to the inferior border of the genu and splenium of the corpus callosum. Additionally, high-resolution imaging in a 2.2 cm thick axial slab of interest that included the thalamus, corpus striatum and parts of the frontal, parietal, temporal and occipital lobes was performed.
The following scan protocol was used:
-
Whole brain three-dimensional (3D) T1-weighted images with a scan duration of 12 min; repetition time (TR)/echo time (TE)/flip angle (FA) = 19 ms/9.2 ms/8°, 280 slices, 210×169 mm field of view, 700×563 matrix size—resulting in a nominal resolution of 0.3×0.3×0.5 mm.
-
Whole brain 3D T2*-weighted gradient echo images with a scan duration of 5 h and 46 min; TR/TE/FA = 24 ms/15 ms/15°, 280 slices, 220×182 mm field of view, 368×303 matrix size—resulting in a nominal resolution of 0.6×0.6×0.5 mm.
-
Whole brain two-dimensional (2D) T2-weighted turbo spin echo images with a scan duration of 6:04 min; TR/TE/FA =14 000 ms/105 ms/90°, slice thickness 3.0 mm with a 0.3 mm interslice gap, 40 slices, 230×182 mm field of view, 384×288 matrix size—resulting in a nominal resolution of 0.6×0.6×3.0 mm.
-
Slice-of-interest high-resolution imaging: 2D T2*-weighted gradient echo images with a scan duration of 9:25 min; TR/TE/FA = 720 ms/21 ms/45°, slice thickness 1.0 mm with a 0.1 mm interslice gap, 20 slices, 240×180 mm field of view, 1000×750 matrix size—resulting in a nominal resolution of 0.24×0.24×1.0 mm (adapted from Duyn and coworkers6). The phase images were subsequently unwrapped using a homodyne filter with a size of 92×92, using a Fourier-based approach, based on the fact that unwanted phase variations are of lower spatial frequency than anatomical information.7 Care was especially given to the filter size. It was set to be large enough to remove all the phase wraps. Since measurements of phase values can be influenced by the settings of the phase unwrapping, the same settings were used for all subjects.
-
Slice-of-interest high-resolution imaging: 2D T2-weighted turbo spin echo images with a scan duration of 9:09 min; TR/TE/FA =3000 ms/58 ms/110°, slice thickness 1.0 mm with a 0.1 mm interslice gap, 20 slices, 240×180 mm field of view, 480/360 matrix size—resulting in a nominal resolution of 0.5×0.5×1.0 mm.
MRI analysis
Before analysing diffuse iron deposition, the magnitude images of the T2*-weighted scans were first inspected for the possible presence of microbleeds since they may interfere with measurements of diffuse iron deposition. Analysis was done by an observer who was blinded to patient data.
Microbleeds were defined as focal areas of signal loss on the whole brain T2*-weighted images with a round or ovoid shape, that did not appear in successive slices, showed a blooming effect on T2*-weighted images and that were devoid of signal hyperintensity on T1- or T2-weighted spin-echo images.8 The number and location of focal areas of signal loss were counted on a digital workstation.
To analyse diffuse iron accumulation, we first inspected the magnitude images of the T2*-weighted images visually for diffuse areas of signal loss. Diffuse hypointensities in the basal ganglia and thalamus were assessed using a subjective two-point scale, and were scored as being present or absent.
To further quantify the amount of diffuse iron accumulation, we used the unwrapped phase images, since they provide a measure of iron content, that is, relatively independent of other tissue characteristics, such as gliosis, water content, etc.1 ,9–12 We measured mean phase shift on the unwrapped phase images of the high-resolution multi-slice T2*-weighted gradient scans after manually outlining regions of interest (ROIs) bilaterally in the globus pallidus, putamen, head of caudate nucleus, thalamus and in the cortex and subcortical white matter of the frontal, temporal, parietal and occipital lobes. Focal areas of phase shift, attributable to cerebral microbleeds or areas of calcifications, were excluded from the ROIs. ROIs in deep grey nuclei were drawn on the slice that best visualised the structure and followed the shape of the structure. ROIs in cortical grey matter and subcortical white matter were drawn on five different slices, each 4 mm apart. ROIs in cortical grey matter consisted of five circular ROIs randomly distributed per lobe per slice. ROIs in subcortical grey matter consisted of one circular ROI per lobe per slice. Mean phase shift in all ROIs was measured on a digital workstation.
Postmortem MRI examinations
Formalin-fixed, approximately 10 mm thick, coronal hemispheric brain slices from another three patients with CADASIL (patient 1: woman, 58 years old; patient 2: man, 64 years old; patient 3: woman, 60 years old) were investigated, which included the basal ganglia and thalamus (n=2), white matter (n=3) and cortex (n=3). Fixation duration ranged from 8 to 11 years. In all cases, informed consent was obtained from the patient or family to perform autopsy and to use the tissues for research purposes. The diagnosis was genetically confirmed and neuropathological findings in these patients were consistent with the diagnosis of CADASIL.
The brain specimen was placed between two perspex plates (170 mm long, 80 mm broad) adjusted to the thickness of the brain slice. Ten holes per plate of 25 mm in diameter were made to allow air bubbles to escape. The brain specimen between the plates was positioned in a plastic container (190 mm long, 85 mm broad, 90 mm high) filled with formalin and was shaken by hand to remove most of the air bubbles. The plastic container was fixed in the head coil using cushions. MRI was performed with the same whole body human 7 T MR system (Philips Healthcare, Best, the Netherlands).
The following scan protocol was used (adapted from van Rooden and coworkers11):
-
High-resolution 0.18×0.18×0.18 mm 3D T2*-weighted gradient echo images with a scan duration of 6 h and 42 min (number of sample averages (NSA)=12); TR/TE/FA = 60 ms/25 ms/10°, slice thickness 0.18 mm, 62 slices, 180×99 mm field of view, 1000×552 matrix size—resulting in a nominal resolution of 0.18×0.18×0.18 mm.
-
High-resolution 0.18×0.18×0.18 mm 3D T1-weighted gradient echo images with a scan duration of 14 h and 5 min (NSA=32); TR/TE/FA = 30 ms/4.9 ms/50°, slice thickness 0.18 mm, 61 slices, 180×99 mm field of view, 1000×552 matrix size—resulting in a nominal resolution of 0.18×0.18×0.18 mm.
-
High-resolution 0.3×0.3×0.3 mm 3D T2-weighted spin echo images with a scan duration of 9 h and 32 min (NSA=2); TR/TE/FA 1000 ms/50 ms/90°, slice thickness 0.3 mm, 37 slices, 180×99 mm field of view, 600×333 matrix size—resulting in a nominal resolution of 0.3×0.3×0.3 mm.
Because of the small number of postmortem scans available, we analysed the scans by visual inspection for diffuse areas of signal loss in cortex, white matter and deep grey nuclei on magnitude images, rather than performing quantitative phase shift analysis. Diffuse hypointensities were scored as being present or absent. Analysis was performed on a digital workstation.
Histopathological analysis
After imaging, the formalin-fixed coronal hemispheric brain slices were embedded in paraffin and cut into 10 μm thick sections. Sections were stained with H&E or Luxol fast blue for routine histopathological examination. Perl's staining was used to identify iron and von Kossa's staining was used to identify calcium. Location and pattern of iron deposition and calcium deposits were recorded. Differences in staining severity of the various areas were assessed qualitatively.
Statistics
Statistical analysis was performed using the SPSS V.16 statistical software package. Differences in age and sex between NOTCH3 MCs and controls were analysed using Student's t tests and χ2 tests. Differences in prevalence of diffuse hypointensities in cortex, white matter and deep grey nuclei in MCs and controls were analysed using Fisher's exact test. Differences in mean phase shift between MCs and controls, and between symptomatic MCs and asymptomatic MCs, were compared using Student's t test, with or without equal variance assumption. Homogeneity of variances of phase shift values between the MC and control group were tested using Levene's test. Significance thresholds were set at p<0.01 to correct for multiple testing. Mean phase shifts were additionally correlated with age using the Pearson correlation coefficient.
Results
Age and sex distribution of MCs (12 men and 13 women; mean age: 46.5 years, SD: 12.2) and controls (10 men and 8 women; mean age: 45.8 years, SD: 12.8) did not differ between groups. The average disease duration of the 14 symptomatic MCs was 7.7 years (range 1–21 years).
In vivo MRI
Focal areas of signal loss on magnitude images
Eleven MCs (44%) had microbleeds, mostly (69%) in the thalamus, but also in the basal ganglia (9%), subcortical white matter (8%), infratentorial brain (7%), cortex (4%) and deep white matter (3%). The number of microbleeds per patient ranged from 1 to 27 (mean 6.8).
Diffuse areas of signal loss on magnitude images
Compared with controls, the MCs had a higher prevalence of diffuse areas of signal loss in the putamen (15/25 MCs, 4/18 controls, p=0.03) and caudate nucleus (11/25 MCs, 1/15 non-MCs, p=0.04). The prevalence of diffuse areas of signal loss did not differ between MCs and non-MCs in the globus pallidus (13/25 MCs, 9/18 controls, p=1.00) and thalamus (2/25 MCs, 0/18 controls, p=0.50). No diffuse areas of signal loss were identified in the white matter or cortex of MCs or controls.
The prevalence of diffuse areas of signal loss was higher in symptomatic MCs than in asymptomatic MCs in the putamen (10/14 symptomatic MCs and 5/11 asymptomatic MCs) and caudate nucleus (7/14 symptomatic MCs and 4/11 asymptomatic MCs). However, these differences were not statistically significant (p>0.05).
Analysis of phase shift on phase images
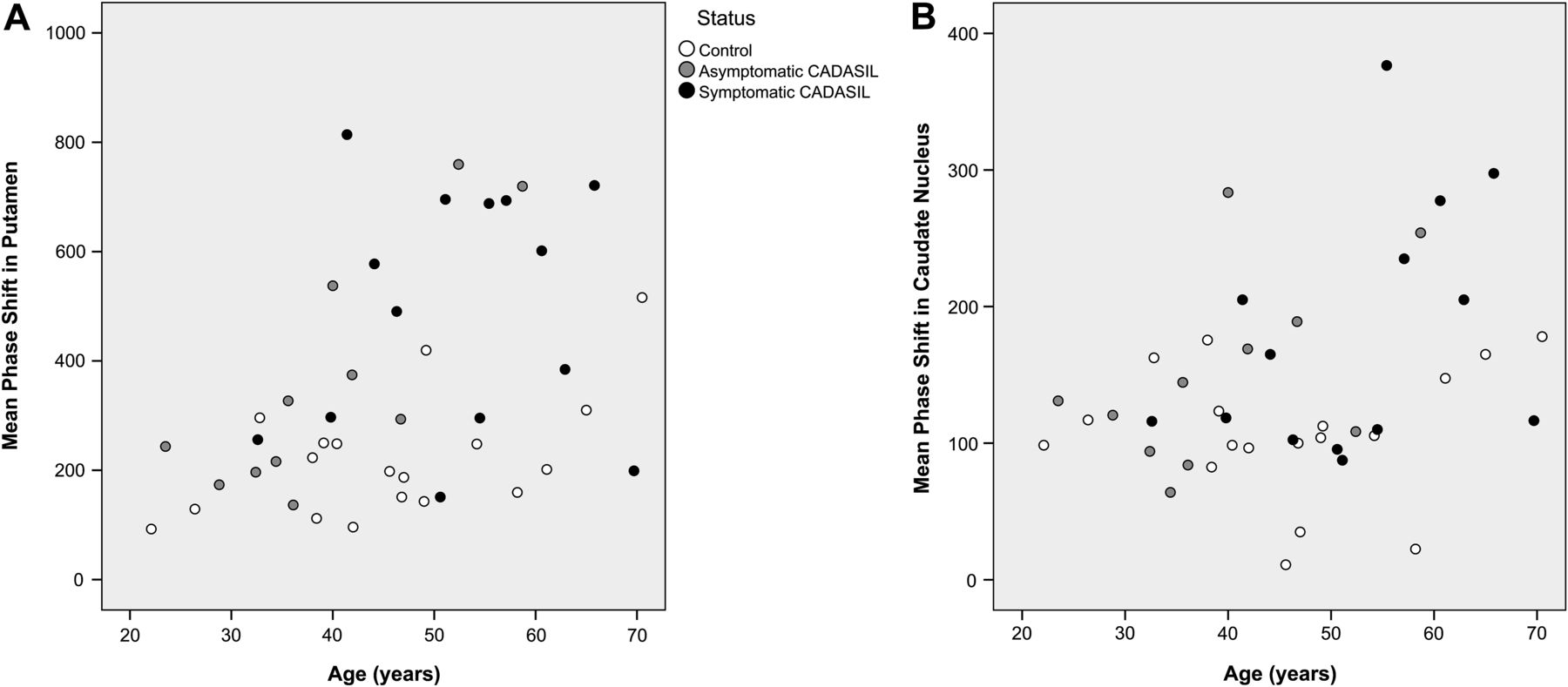
MCs demonstrated a symmetrically (Pearson correlation coefficient >0.8) increased phase shift compared with controls in the putamen (p=0.0002) and caudate nucleus (p=0.006) (table 1, figure 1, figure 2A,B). Phase shift values in these nuclei also showed significantly more variation within the MC group than in the control group. The amount of phase shift in the globus pallidus and thalamus (table 1) and in the cortex and subcortical white matter did not differ between mutation carriers and controls.
Mean phase shift in deep grey nuclei

T2*-weighted gradient echo scans: magnitude images (top row) and unwrapped phase images (bottom row) of a 60-year-old patient with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) (left) and a 60-year-old control subject (right), showing increased signal loss and phase shift in the putamen and caudate nucleus of the patient with CADASIL.
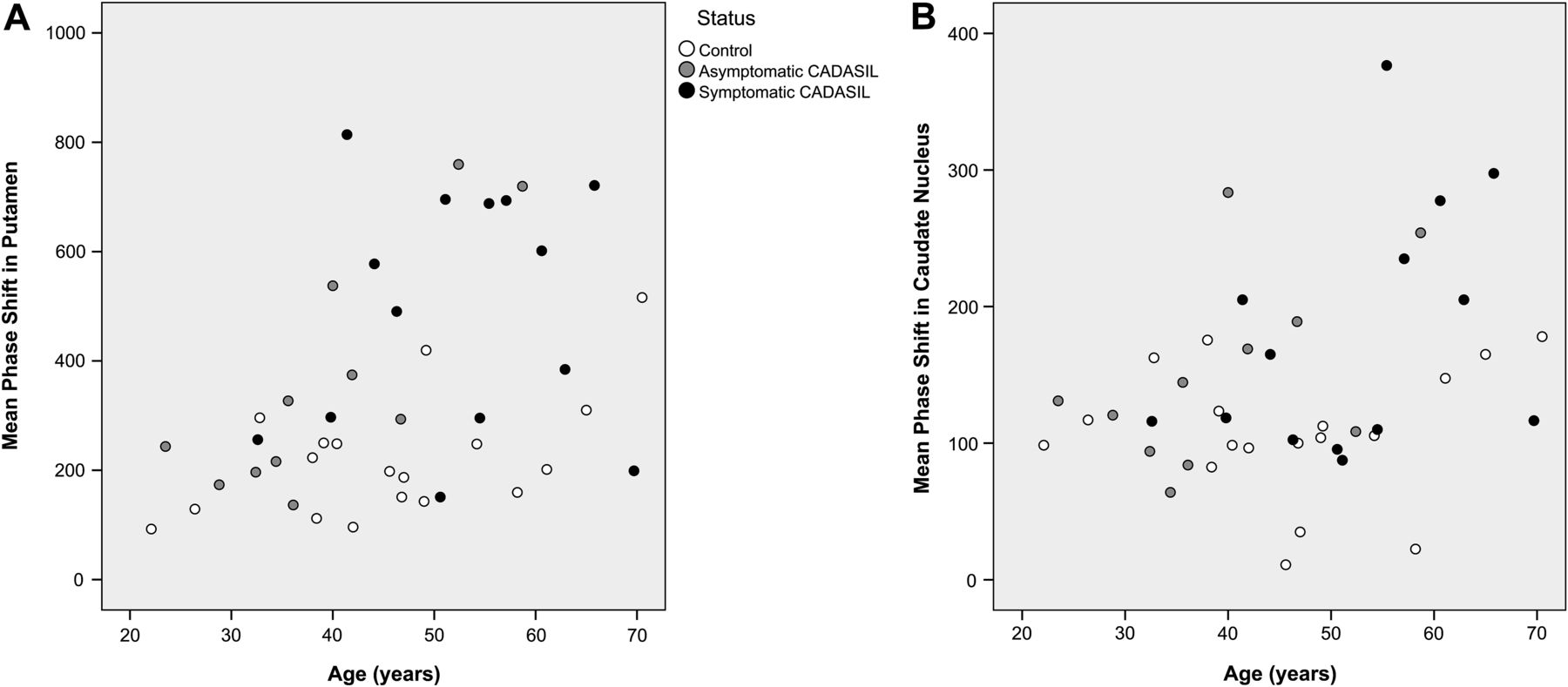
Phase shift in putamen (A) and caudate nucleus (B) in mutation carriers and controls. CADASIL, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy.
Symptomatic MCs had higher mean phase shift values in the putamen and caudate nucleus than asymptomatic MCs (symptomatic MCs: putamen =0.490 rad, caudate nucleus =0.179 rad; asymptomatic MCs: putamen =0.361 rad, caudate nucleus =0.149 rad). However, these differences were not statistically significant. Similarly, no significant differences in phase shift were found between symptomatic and asymptomatic MCs in the globus pallidus, thalamus, cortex and subcortical white matter.
In MCs an increased phase shift in the putamen and caudate nucleus was associated with higher age (putamen: B =0.008 rad per year, r=0.47, p=0.02; caudate nucleus: B=0.003 rad per year, r=0.45, p=0.02). In the healthy controls an increased phase shift in the putamen was associated with higher age (B=0.005 rad per year, r=0.55, p=0.02). No association was found between age and phase shift in putamen and caudate nucleus in controls.
Postmortem MRI and histopathological analysis
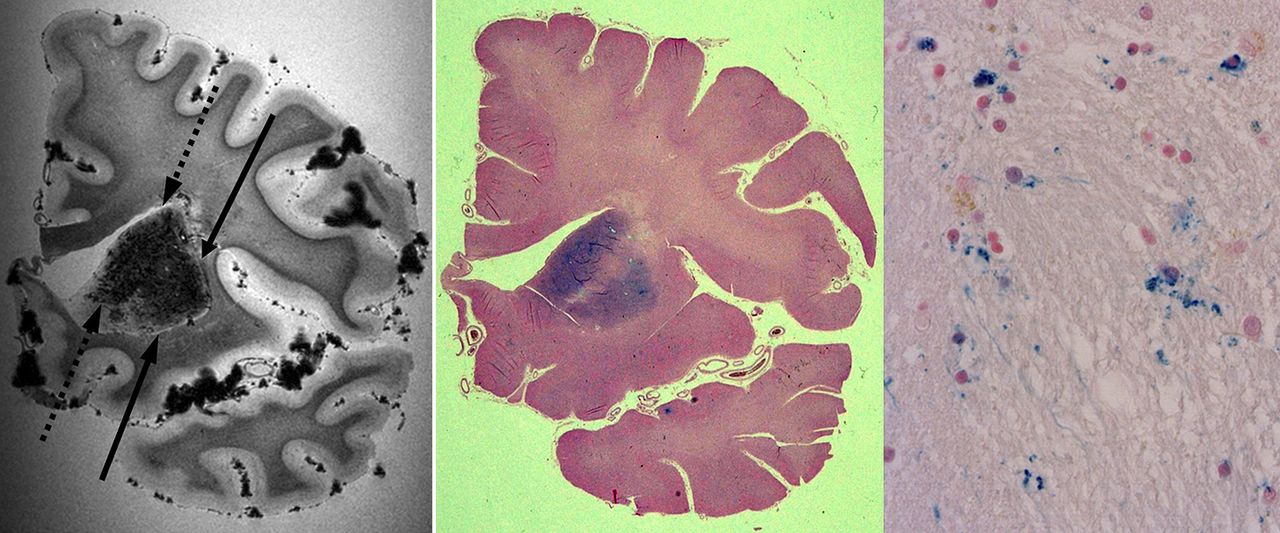
Visual inspection of the postmortem MRI scans revealed marked diffuse signal loss in the putamen and caudate nucleus and to a lesser extent in the globus pallidus of the brain specimens (figure 3).
{kind=link}
{kind=link}
{kind=link}
MRI and histopathological iron staining of postmortem brain tissue of a patient with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Left: T2*-weighted gradient echo MRI scan showing signal loss in the putamen (solid arrows) and caudate nucleus (dashed arrows). Middle: iron staining of the same slice shows iron staining in the putamen and caudate nucleus. Right: detail of the iron stain from the putamen (40× magnification) shows iron deposition in a perivascular and diffuse distribution.
Iron histochemistry of the brain specimens revealed macroscopic evidence of iron deposition in the caudate nucleus and putamen and to a lesser extent in the globus pallidus. The pattern of iron staining matched the pattern of signal loss visible on postmortem MRI (figure 3). No iron staining was observed macroscopically in the cerebral cortex (except for a remnant of a haemorrhage in the temporal cortex of one patient), the subcortical white matter or the thalamus.
Microscopy showed that the iron deposits in the caudate nucleus and putamen were located scattered throughout the parenchyma and perivascularly, and that they were mostly associated with cells with morphology of glia. Microscopy also showed mild diffuse staining of myelin in the subcortical white matter, with delicate patches of cell-associated iron deposits. No microscopic iron deposits were found in the thalamus or in the cortex.
Von Kossa staining revealed sporadic calcium deposits in the globus pallidus, putamen and caudate nucleus. This calcium staining was mild and did not match the pattern of MRI hypointensities.
Discussion
This combined MRI and histopathological study shows that patients with the small vessel disease CADASIL have diffuse areas of increased hypointensity and phase shift in the putamen and caudate nucleus, which we show to be caused by progressive local iron accumulation.
Increased iron accumulation has not been demonstrated before in CADASIL or in other forms of small vessel disease, but has mainly been associated with neurodegenerative diseases such as Alzheimer's and Huntington disease, with large vessel stroke and with normal ageing.1 ,9–12 The findings in this article suggest that chronic microvascular brain disease could also be an important component of iron deposition in the general ageing population.
The mechanism that leads to this iron deposition in CADASIL remains to be determined. Possibly, the deposition of iron molecules is a consequence of secondary neurodegeneration. Possibly, the demyelination of white matter tracts and the atrophy of cerebral cortex lead to a decreased demand of iron from the storage place in the deep grey nuclei, causing chronic accumulation of iron in the striatum.13
The effects of the increased iron levels in deep brain nuclei in this study population are unknown. In general, increased brain iron levels may lead to cerebral damage by interfering with protein synthesis or by increasing the vulnerability to oxidative stress.14 ,15 In CADASIL, this may lead to worsening of clinical symptoms and to faster clinical disease progression. In our study symptomatic patients with CADASIL had higher values of phase shift than asymptomatic MCs, which suggests that iron deposition is associated with disease severity. However, since these differences were not statistically significant, it remains unclear whether this association is true. Studies with a larger sample size need to be performed to confirm the relation between iron deposition and clinical disease severity in CADASIL. Eventually, the present findings could open new venues to modify the course of the disease in CADASIL, for example, by using iron chelators or inhibitors of oxidative stress.
It should be noted that even though a significant overall difference was found, many MCs showed phase shift values that were still comparable to those of the controls. However, in the MC group the variance of phase shift values was larger than that in the control group, especially at higher age. Part of the overall difference can be explained by this larger variance in MCs. This large variation in the amount of iron deposition in CADASIL can be considered analogous to the large phenotypical variation in other clinical and MRI findings in CADASIL.16
We measured iron deposition indirectly by detecting signal loss on magnitude images and measuring increased phase shift on phase images, and not by direct measurement of iron concentration, which is still an area of contention in terms of quantitation using MRI. Causes of decreased signal intensity other than iron, such as calcifications or depositions of other types of metal, cannot be ruled out on the MRI scans. However, histopathological analysis showed that the pattern of hypointensity observed on MRI matches the pattern of iron staining on histochemistry.
This study was performed using a 7 T MRI scanner, which is considered to be more sensitive to iron deposition than MRI scanners with standard field strengths.6 However, since the iron deposition in this study was distributed diffusely in relatively large anatomical structures, it is likely that this process of iron deposition can also be studied using MRI scanners with standard field strengths.
In conclusion, high-field MRI demonstrates progressive diffuse areas of T2* hypointensity and phase shift in the striatum in CADASIL, indicating that progressive iron deposition is associated with the pathology of CADASIL, and possibly of other small vessel diseases. Further research is needed to elucidate the underlying pathophysiology and possible implications.
References
Footnotes
-
Competing interests None.
-
Ethics approval Ethics approval was provided by Medical ethics committee of the Leiden University Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.