Article Text

Abstract
Objectives To determine if urinary biomarkers of effect and potential harm are elevated in electronic cigarette users compared with non-smokers and if elevation correlates with increased concentrations of metals in urine.
Study design and setting This was a cross-sectional study of biomarkers of exposure, effect and potential harm in urine from non-smokers (n=20), electronic cigarette users (n=20) and cigarette smokers (n=13). Participant’s screening and urine collection were performed at the Roswell Park Comprehensive Cancer Center, and biomarker analysis and metal analysis were performed at the University of California, Riverside.
Results Metallothionein was significantly elevated in the electronic cigarette group (3761±3932 pg/mg) compared with the non-smokers (1129±1294 pg/mg, p=0.05). 8-OHdG (8-hydroxy-2′-deoxyguanosine) was significantly elevated in electronic cigarette users (442.8±300.7 ng/mg) versus non-smokers (221.6±157.8 ng/mg, p=0.01). 8-Isoprostane showed a significant increase in electronic cigarette users (750.8±433 pg/mg) versus non-smokers (411.2±287.4 pg/mg, p=0.03). Linear regression analysis in the electronic cigarette group showed a significant correlation between cotinine and total metal concentration; total metal concentration and metallothionein; cotinine and oxidative DNA damage; and total metal concentration and oxidative DNA damage. Zinc was significantly elevated in the electronic cigarette users (584.5±826.6 µg/g) compared with non-smokers (413.6±233.7 µg/g, p=0.03). Linear regression analysis showed a significant correlation between urinary zinc concentration and 8-OHdG in the electronic cigarette users.
Conclusions This study is the first to investigate biomarkers of potential harm and effect in electronic cigarette users and to show a linkage to metal exposure. The biomarker levels in electronic cigarette users were similar to (and not lower than) cigarette smokers. In electronic cigarette users, there was a link to elevated total metal exposure and oxidative DNA damage. Specifically, our results demonstrate that zinc concentration was correlated to oxidative DNA damage.
- electronic cigarettes
- cigarettes
- non-smokers
- metals
- biomarkers
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
Is increased electronic cigarette usage associated with elevated metal exposure and if such exposure can cause biological harm?
What is the bottom line?
Biomarkers of exposure (cotinine and metals), effect (metallothionein) and potential harm (8-isoprostane and 8-OHdG) were elevated in electronic cigarette users and were similar to concentrations in cigarette smokers; also increased electronic cigarette usage (as measured by cotinine) was correlated with elevated urinary metal concentrations, which were correlated with oxidative DNA damage.
Why read on?
This is one of the first studies to demonstrate a correlation between biological harm and electronic cigarette usage, suggesting the metal constituents (in particular zinc) in electronic cigarette aerosol can cause oxidative DNA damage. Given the recent deaths and pulmonary illnesses related to electronic cigarette usage, it is important for readers to know about the potential health effects related to electronic cigarette usage.
Introduction
Cigarette smoking causes more than 480 000 deaths annually in the USA and is the leading cause of preventable death.1 Electronic cigarettes, which grew in usage over 900% between 2011 and 2015, do not burn tobacco and may be a safer product.2 However, there are limited scientific data to prove that electronic cigarettes are actually less harmful than combustible tobacco products, although they may be harmful in different ways. To the contrary, some previous research has demonstrated that electronic cigarette aerosols contain potentially harmful chemicals, such as acrolein; formaldehyde and benzene3; cytotoxic flavour chemicals, such as diacetyl and cinnamaldehyde4 5; metals and ultrafine particles including tin, chromium and nickel nanoparticles6 7; and free radicals.8 Moreover, some electronic cigarette refill fluids and aerosols showed cytotoxicity when tested in vitro,9 10 an effect that has been linked to metals in the refill fluid.6 An in vitro study demonstrated that isolated human alveolar macrophages exposed to electronic cigarette vapour induces inflammation and reduces phagocytosis leaving the patient more susceptible to pulmonary infections.11 Moreover, recent case reports have attributed electronic cigarette use to several adverse health effects, such as respiratory diseases,12 increased risk for cardiovascular disease13 and impaired wound healing after surgery.14 Several previous studies on electronic cigarettes have evaluated biomarkers of exposure in blood, urine and saliva,15–17 but none has yet examined and quantified biomarkers of effect and potential harm in relation to metals in electronic cigarette users.
This study compares urinary biomarkers of exposure, effect and potential harm in non-smokers, conventional cigarette smokers and electronic cigarette users and accounts for the effect of gender and age on biomarker expression. Based on the above studies, we hypothesised that there would be an increase in the level of biomarkers of effect and potential harm in electronic cigarette users compared with non-smokers and a decrease compared with cigarette smokers. The urinary biomarker of effect, metallothionein, is a protein that responds to and protects against metal toxicity and free radical stress. Urinary biomarkers of potential harm were two markers of oxidative stress: (1) 8-isoprostane, a prostaglandin formed by fatty acid peroxidation, and (2) 8-OHdG, a product of DNA oxidation. Urinary biomarkers of exposure were: (1) cotinine, a nicotine metabolite to measure smoking or vaping usage, and (2) total concentration of 11 urinary metals, which are present in electronic cigarette aerosol6 7 18 and are known to associate with metallothionein.19 20 Regression analyses were performed to identify relationships between biomarkers of exposure (cotinine and metals), effect (metallothionein) and potential harm (8-OHdG). To isolate the observed oxidative effects to a specific metal, regression analyses were performed between the urinary concentrations of individual metals and 8-OHdG.
Materials and methods
Subjects
The urine samples were from participants who were non-smokers, cigarette smokers and electronic cigarette users. Participants were recruited through local media and flyers posted in various locations around the Buffalo, New York area. Potential participants were provided with a brief description of the study and had an opportunity to ask questions about the study procedures. All potential participants were screened over the phone for inclusion and exclusion criteria. The exclusion criteria included concurrent use of smokeless tobacco, pipes or cigars; alcohol or illicit drug dependence within the past 6 months or current illicit drug use (including marijuana; self-reported); psychiatric illness; and use of nicotine replacement therapy. Information about medication and vitamins/antioxidants/metal usage was not collected. All eligible subjects who had been asked to come to the clinic for screening were given an informed consent form to read and sign. Copies of the signed consent forms were given to the research subject and were also stored in a secure location, along with the participant’s research chart. Informed written consent was obtained from each participant prior to their participation. Eligible participants were then asked to come to Roswell Park Comprehensive Cancer Center for a one-time visit, which lasted approximately 1 hour. Spot urine samples were collected during this on-site visit. The Roswell Park Institutional Review Board (IRB) had reviewed all procedures prior to implementation (protocol number I 247313).
A total of 53 participants were gender matched and age matched and selected for biomarker analysis. Because age may affect the basal expression level of biomarkers, the subjects were separated into those ≤40 years old and ≥41 years old, with the groups containing 23 and 30 samples, respectively. Out of these age-separated samples, participants were selected from the non-smoker, cigarette smoker, and electronic cigarette user groups. Each group had approximately equal male and female samples. Using a one-way analysis of variance (ANOVA) and a Tukey’s multiple comparison test, there were no significant differences in the ages of the younger participants or in the ages of the older participants; however, the ages of the younger and older groups were significantly different from each other. There were negligible levels of 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) in the non-smokers (2.8±6.3 pg/mg of creatinine) and electronic cigarette users (13.3±18.6 pg/mg of creatinine) indicative of no tobacco use, in contrast to the cigarette smokers (105.7±87.4 pg/mg of creatinine) who had significantly elevated NNAL (online supplementary figure 1). In the non-smokers, no samples had levels of cotinine ≥1.0 ng/mg (online supplementary figure 2), confirming smoking abstinence. The demographics of the 53 participants who provided urine samples were organised by age, gender and smoking group (table 1).
Supplemental material
Demographics of the 53 participants included in this study separated by smoking group, age and gender
Biospecimen collection
Spot urine samples were collected from participants in a previous study,16 and cotinine, NNAL and creatinine concentrations were determined at the Centers for Disease Control and the Roswell Park Comprehensive Cancer Center (RPCCC), respectively. Aliquots of 45 mL of fresh urine samples were transferred to 50 mL Falcon tube, then centrifuged and immediately frozen at −20°C and stored at the RPCCC laboratory. Prior to shipping, samples were thawed, and 1.5 mL aliquots were transferred to smaller tubes and shipped frozen to University of California, Riverside for biomarker analysis.
Selection of biomarkers
Biomarkers were selected by studying previous literature pertaining to urinary biomarkers in smokers.21–25 The selection criteria for our panel of urinary biomarkers was based on our goal to analyse metal exposure and oxidative stress (table 2). To evaluate exposure, cotinine and metals were measured in urine samples. Metallothionein, which increases when metal exposure is elevated, was used as a biomarker of effect. Conventional cigarettes and electronic cigarettes generate free radicals that cause cellular oxidative stress.8 26 27 Therefore, oxidative damage was evaluated in the three study groups by measuring urinary 8-isoprostane (a biomarker of lipid peroxidation) and 8-OHdG (a biomarker of DNA oxidation). Cigarette smoke and electronic cigarette aerosols contain a mixture of metals6 7 28 that could lead to an increased production of metallothionein (a metal exposure and reactive oxygen species (ROS) scavenging biomarker), which is a cysteine-rich protein that functions in metal binding.25 All selected biomarkers described above have been shown to be specifically associated with clinically relevant outcomes and diseases (table 2).
Clinical diseases associated with biomarkers measured in this study
Urinary creatinine concentrations
Spot urine samples were used since biomarkers would not necessarily be stable in samples collected over 24 hours. Because spot urine samples were used, it was necessary to normalise the data to creatinine, which is relatively stable in concentration over time. Creatinine concentrations in urine were analysed at the RPCCC clinical laboratory in Buffalo. There were no significant differences in creatinine concentrations in relation to gender or age (online supplementary figure 3).
Biomarker of exposure (cotinine, NNAL and metal concentration) analysis
Cotinine and NNAL were measured using previously published29 30 and fully validated methods. Eleven elements/metals (antimony, cadmium, copper, indium, lead, nickel, rubidium, selenium, silver, titanium and zinc) in urine samples were measured by inductively coupled mass spectrometry and used to calculate total urinary metal concentration. The 11 metals were selected for analysis because they have all been identified in electronic cigarette aerosols and are known to associate with metallothionein. There was no significant elevation of the total 11 metals in the smoking groups, though it is slightly elevated in the electronic cigarette group (online supplementary figure 4). Details of metal analysis are given in the online supplementary information.
Biomarkers of effect and potential harm analysis using ELISA
Each ELISA kit was quality tested for accuracy and reproducibility using urine samples collected in house. Samples were tested in duplicate on three different days, and the biomarker concentration was normalised to creatinine. A range of sample dilutions was tested to determine the optimal dilution for quantification of each biomarker from the kits’ standard curves. For all ELISA kits, the coefficient of variation for the three independent experiments was ≤15%, except for metallothionein, which was ≤20%. Any urine sample with a biomarker concentration outside the lowest or highest limit of quantification was excluded for statistical analysis. In all subsequent ELISA analyses, biomarkers were run in duplicate wells for each urine sample.
Following a 1:4 dilution in buffer, urine samples were analysed to determine 8-isoprostane concentration using the Urinary 8-Isoprostane ELISA kit (Detroit R&D, Michigan, USA). The concentration of 8-OHdG was determined using a DNA Damage (8-OHdG) ELISA Kit (Stress Marq Biosciences, Victoria, Canada), following a 1:20 dilution. Urine samples were analysed for metallothionein using a Human Metallothionein ELISA Kit (LifeSpan BioSciences, Washington, USA), following a 1:20 or 1:40 dilution in sample diluent.
Statistical analysis
Two urine samples from the electronic cigarette group had abnormally high creatinine concentrations (≥3 mg/mL) as detected by a statistical outlier test and were removed from further analysis. For each urine sample, the biomarker concentration was normalised to its respective creatinine concentration. Because the normalised biomarker concentration data were not normally distributed, a Box-Cox transformation was performed after which a three-way ANOVA was applied in MiniTab 17.0 (MiniTab Inc, Pennsylvania, USA) using gender, age and smoking group as factors. Outliers were removed if they had a large standardised residual (≥2.0 or ≤−2.0). In all the three-way ANOVA models, the two-way and three-way interactions were not significant, and our final model included age, gender and smoking group. Post hoc tests were used to compare different age groups, gender groups and smoking groups. When the smoking group was analysed independently (disregarding gender and age), a Dunnett’s post hoc test was used with the electronic cigarette group as the main comparison group, and the comparisons were electronic cigarette users versus non-smokers and electronic cigarette users versus cigarette smokers. All linear correlation analyses were performed using the Linear Regression Analysis (R2 and p-value reported) in PRISM 7.0 (GraphPad, California, USA). All graphs reported in this manuscript were made in PRISM 7.0.
Patient and public involvement
No patients were involved in the research planning or design, nor were they involved in any aspect of the study besides urine collection. There are no plans to directly disseminate the results of the research to study participants. The dissemination of results will be achieved through publication or press release.
Results
Biomarker of effect
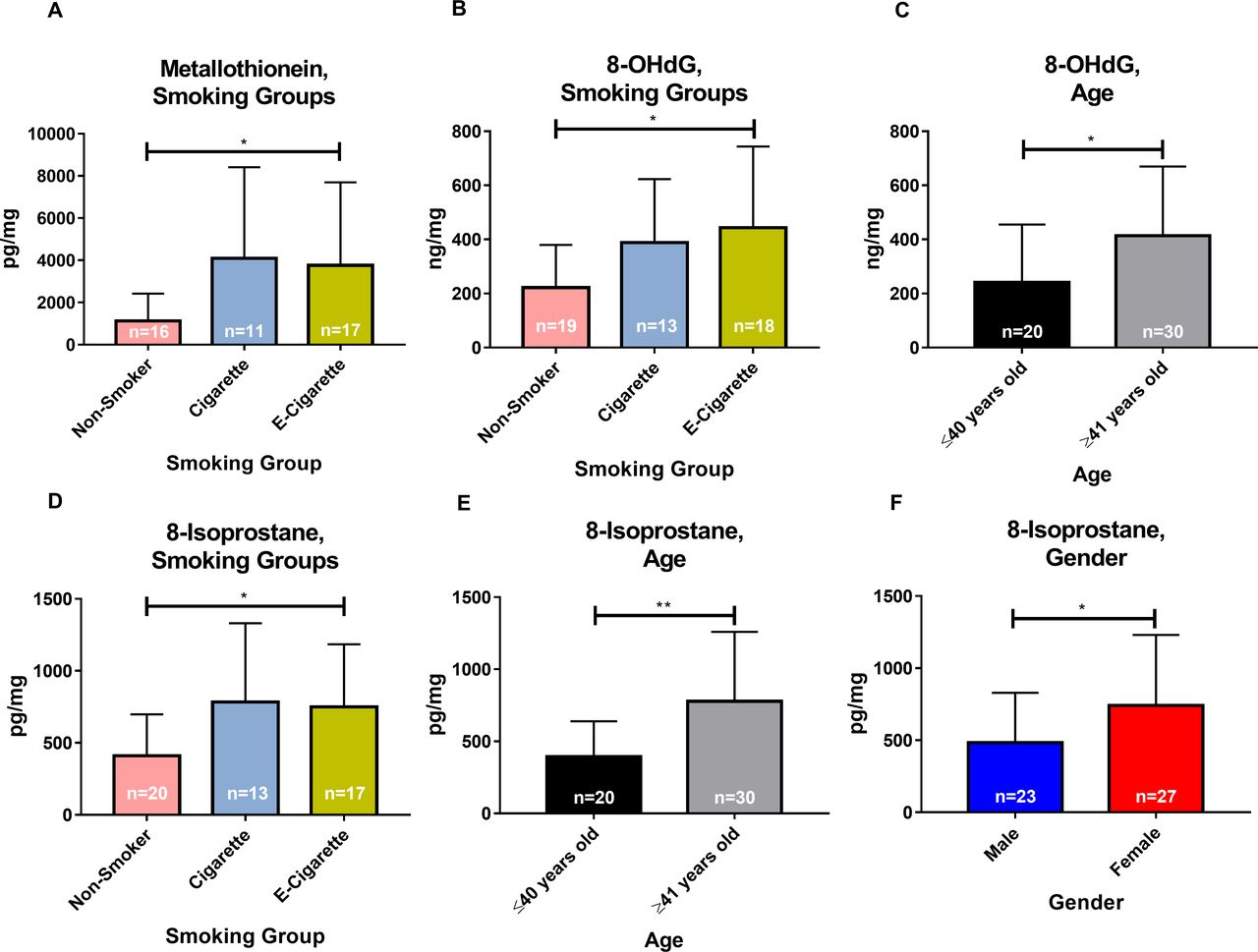
Metallothionein, a biomarker of effect (due to metal and ROS exposure), in the electronic cigarette group (3761±3932 pg/mg) was significantly elevated when compared with the non-smokers group (1129±1294 pg/mg, p=0.05), and these concentrations were similar to the cigarette smokers group (4096±4320 pg/mg, p=0.95) (figure 1A). There were no differences in age or gender.

Urinary metallothionein (pg/mg of creatinine), 8-OHdG (ng/mg of creatinine) and 8-isoprostane (pg/mg of creatinine) are significantly elevated in electronic cigarette users compared with non-smokers. (A) Metallothionein levels among the different smoking groups. (B) 8-OHdG concentration in the different smoking groups. (C) 8-OHdG concentration in the younger and older populations. (D) 8-isoprostane levels among the different smoking groups. (E) 8-Isoprostane levels in the younger and older populations. (F) 8-Isoprostane levels in men and women. Bars are the means and SD for each group. *P<0.05; **p<0.01.
Biomarkers of potential harm (oxidative stress)
A significant elevation in urinary levels of the biomarker of DNA oxidation, 8-OHdG, occurred in electronic cigarette users (442.8±300.7 ng/mg) versus non-smokers (221.6±157.8 ng/mg, p=0.01) (figure 1B). There was no significant difference between electronic cigarette users (442.8±300.7 ng/mg) and cigarette smokers (388±235 ng/mg, p=0.75). Age affected 8-OHdG levels; those ≥41 years old (413.4±256.4 ng/mg) had significantly elevated 8-OHdG compared with those ≤40 years (241.2±214.1 ng/mg, p=0.02) (figure 1C). There was no effect on gender.
The lipid peroxidation biomarker, 8-isoprostane, showed a significant increase in electronic cigarette users (750.8±433 pg/mg) versus non-smokers (411.2±287.4 pg/mg, p=0.03) (figure 1D). There was no significant difference between electronic cigarette users (750.8±433 pg/mg) and cigarette smokers (784.2±546.1 pg/mg, p=0.96). Moreover, the ≥41-year-old population (777.6±481.5 pg/mg) was significantly elevated in 8-isoprostane compared with those ≤40 years (392.6±246.9 pg/mg, p=0.002) (figure 1E). In addition, 8-isoprostane was significantly elevated in women (741.8±489.3 pg/mg) versus men (484.9±345, p=0.04) (figure 1F).
Biomarkers of exposure are correlated with oxidative DNA damage in electronic cigarette users
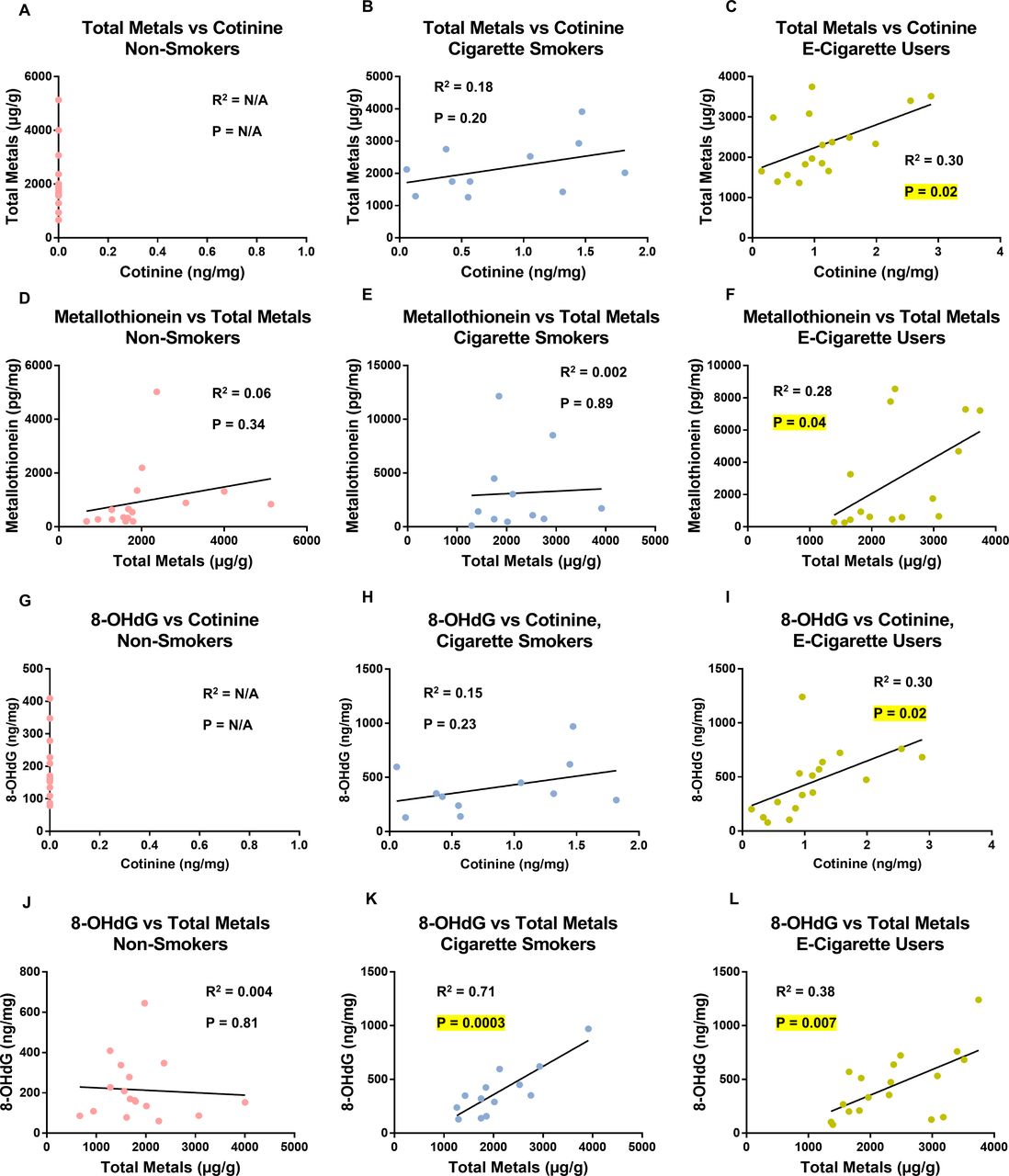
Results of linear regression analyses performed on the non-smokers, cigarette smokers and electronic cigarette users are presented in figure 2 for the following correlations: (1) cotinine and total metal concentration (figure 2A–C), (2) total metal concentration and metallothionein (figure 2D–F), (3) cotinine and 8-OHdG (figure 2G–I) and (4) total metal concentration and 8-OHdG (figure 2J–L). There were no significant correlations in the non-smokers (figure 2A,D,G,J). In the cigarette smokers group, only total metal concentration and 8-OHdG were significant (figure 2K, p=0.0003). In the electronic cigarette users group, all linear regression analyses were significant: cotinine and total metal concentration (figure 2C, p=0.02), total metal concentration and metallothionein (figure 2F, p=0.04), cotinine and 8-OHdG (figure 2I, p=0.02) and total metal concentration and 8-OHdG (figure 2L, p=0.007).
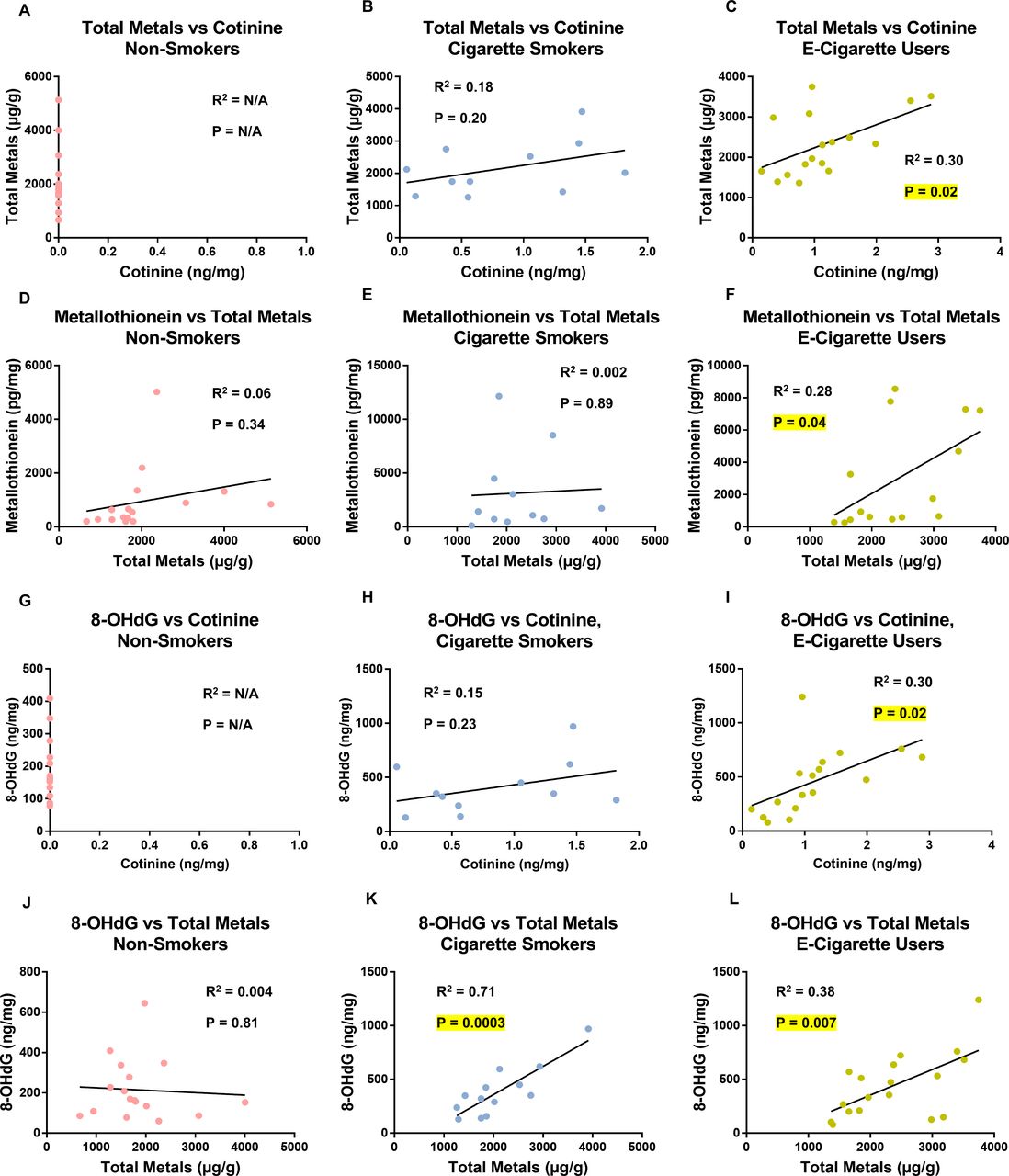
Correlation between total metals and cotinine, metallothionein and total metals, 8-OHdG and cotinine, and 8-OHdG and total metals in urine. (A–C) Linear regression analysis comparing total metal (µg/g of creatinine) and cotinine concentration (ng/mg of creatinine) in urine of the non-smokers, cigarette smokers and electronic cigarette user groups. (D–F) Linear regression analysis comparing metallothionein concentration (pg/mg of creatinine) and total metal concentration (µg/g of creatinine) in urine in the non-smokers, cigarette smokers and electronic cigarette users groups. (G–I) Linear regression analysis comparing 8-OHdG (ng/mg of creatinine) and cotinine (ng/mg of creatinine) concentration in urine of the non-smokers, cigarette smokers and electronic cigarette user groups. (J–L) Linear regression analysis comparing 8-OHdG (ng/mg of creatinine) and total metal (µg/g of creatinine) concentration in urine of the non-smokers, cigarette smokers and electronic cigarette user groups. N/A=not applicable since levels of cotinine in non-smokers was negligible.
Selenium and zinc were elevated in electronic cigarette users
Two of the 11 metals that were analysed were significantly elevated in the electronic cigarette group. Selenium concentrations (figure 3A) were significantly elevated in the electronic cigarette users (54±20.6 µg/g) compared with non-smokers (41.8±14.1 µg/g, p=0.04) and cigarette smokers (39.7±17.3 µg/g, p=0.05). Zinc concentrations (figure 3B) were significantly elevated in electronic cigarette users (584.5±826.6 µg/g) compared with non-smokers (413.6±233.7 µg/g, p=0.03). Zinc in the electronic cigarette users was not significantly elevated when compared with cigarette smokers (470.7±223.6 µg/g, p=0.17).
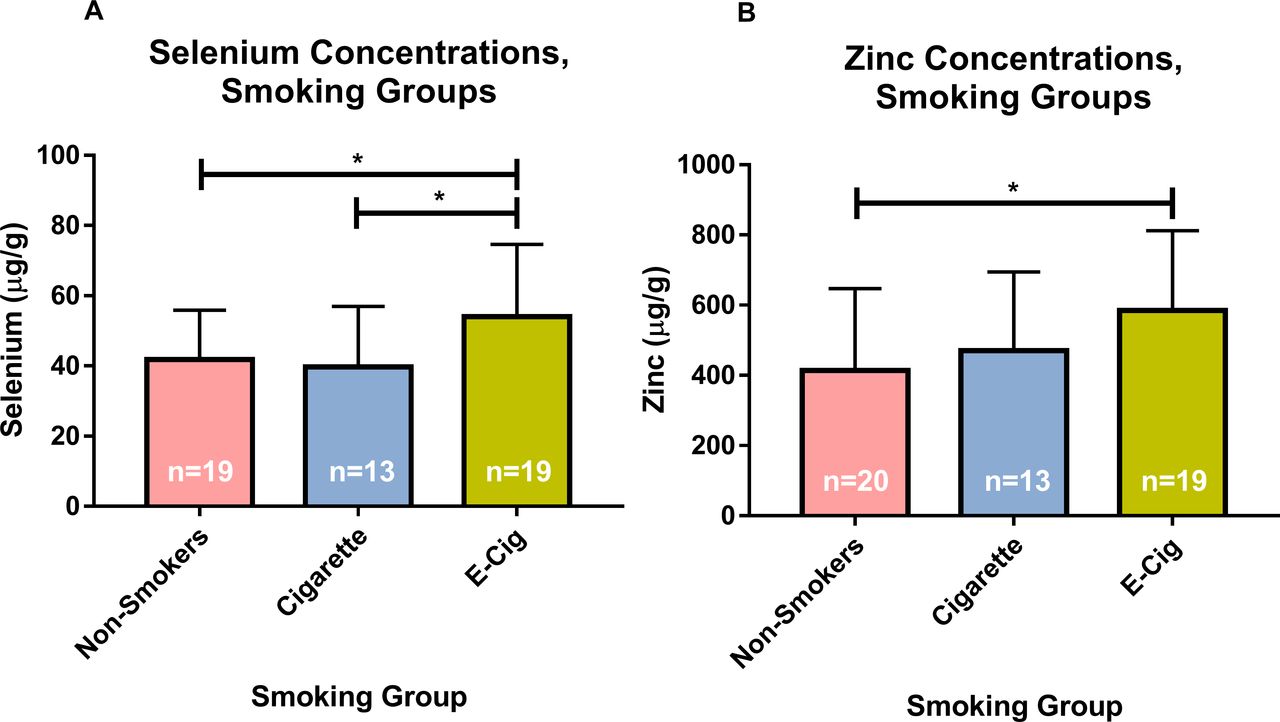
Urinary selenium (µg/g of creatinine) and zinc (µg/g of creatinine) concentrations are significantly increased in the electronic cigarette users. (A) Selenium concentrations in the different smoking groups. (B) Zinc concentrations in the different smoking groups. Bars are the means and SD for each group. *P<0.05.
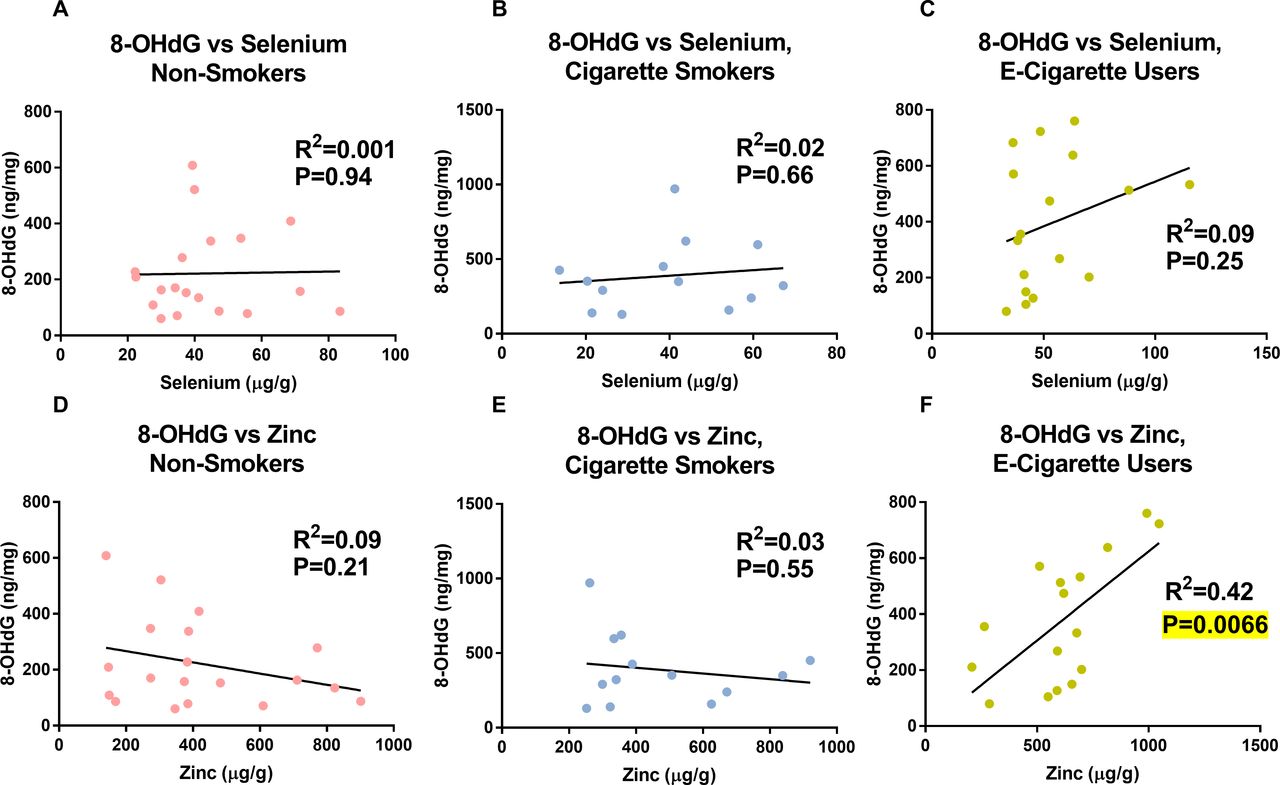
Zinc was correlated with oxidative DNA damage in electronic cigarette users
Regression analyses were performed to compare urinary concentrations of selenium and zinc to 8-OHdG in the non-smokers, cigarette smokers or electronic cigarette users (figure 4). There were no significant correlations for selenium versus 8-OHdG (figure 4A–C). In the electronic cigarette users only, zinc was significantly correlated to 8-OHdG (p=0.0066) (figure 4F). In non-smokers and cigarette smokers, zinc was not correlated to 8-OHdG (figure 4A,B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Zinc concentrations (µg/g of creatinine) are significantly correlated to oxidative DNA damage in the electronic cigarette users. (A–C) Linear regression analysis comparing selenium (µg/g of creatinine) and 8-OHdG (ng/mg of creatinine) in urine of the non-smokers, cigarette smokers and electronic cigarette user groups. (D–F) Linear regression analysis comparing zinc (µg/g of creatinine) and 8-OHdG (ng/mg of creatinine) in urine in the non-smokers, cigarette smokers and electronic cigarette users groups.
Discussion
Consistent with our hypothesis, our study shows for the first time that biomarkers of effect and potential harm were elevated in the urine of the electronic cigarette users compared with non-smokers. Moreover, in electronic cigarette users, the levels of biomarkers of effect and potential harm were positively correlated with biomarkers of exposure to nicotine and metals. Importantly, electronic cigarette participants in our study did not report using other tobacco products and were not dual users of electronic cigarettes and conventional cigarettes. Before entering our study, all electronic cigarette users who were previous cigarette smokers had abstained from smoking cigarettes for a minimum of 6 months, and abstinence was confirmed by undetectable NNAL (online supplementary figure 1). Previous literature has shown that abstinence from cigarette smoking was concurrently linked to a decrease in levels of 8-isoprostane and 8-OHdG, which returned to non-smokers levels.31 Taken together, the above information supports the conclusion that the elevation of 8-isoprostane and 8-OHdG in urine was associated with electronic cigarette use specifically. Surprisingly, we did not find a significant reduction in biomarkers of effect and potential harm between electronic cigarette users and cigarette smokers. This observation may be explained by the fact that electronic and conventional cigarettes and their aerosols have anatomical, chemical and particulate differences, which may contribute to physiological harm in separate ways.
Cigarette smoke and electronic cigarette aerosol contain a mixture of metals and free radicals6–8 28 32 that could be contributing to the oxidative harm in our participants. The metals in electronic cigarette aerosols come mainly from the metal components in the atomiser and the e-fluid that is heated in the atomiser.7 33 Metal concentration in urine was positively correlated with cotinine concentration, indicating that metals were elevated with increased aerosol exposure.
Metal increase in urine is further supported by the observed elevation in metallothionein, which acts as a heavy metal-binding protein and also protects cells from oxidative stress by scavenging ROS .25 Metallothionein normally binds physiological metals, such as zinc and copper, but can also bind xenobiotic heavy metals such as cadmium, silver and arsenic25 34 that are present in cigarette smoke35 and electronic cigarette aerosols.7 Metallothionein can also associate with at least 20 different elements/metals,19 20 and 11 of these have been found in cigarette smoke28 36 or electronc cigarette aerosol6 7 18 and were present in the urine of our participants. The increase in metallothionein in the electronic cigarette user group was positively correlated with increasing metal concentration in their urine and was likely a response to metals inhaled by the electronic cigarette users. In cigarette smokers, metallothionein was not significantly correlated with increasing metal concentration, suggesting other factors such as ROS may be contributing to its activation. Also, cigarette smoke can have a different composition of metals than electronic cigarette aerosol,6 7 18 28 36 which were not selected for in our 11-metal analysis, and therefore, the total metal concentration in smokers was not correlated to cotinine concentration.
Elevation of toxic metals can induce oxidative stress.37 38 In the electronic cigarette group, there was a significant correlation between total metals and oxidative DNA damage. A similar correlation was observed for the cigarette smokers. Lipid oxidation was not significantly correlated with metal concentration in either the electronic cigarette or cigarette smokers groups. There are multiple isoprostanes and isoprostane metabolites formed in vivo during oxidative conditions,39 and we measured only 8-isoprostane, which may account for the lack of correlation between lipid oxidation and metal concentration. In contrast, during DNA oxidation, the guanine residue is highly oxidised compared with the other nucleic bases, leading to the formation of a single DNA oxidation product (8-OHdG), which makes correlation to oxidative stress straightforward.
Both zinc and selenium, which were significantly elevated in the electronic cigarette user group, are present in electronic cigarette aerosols, usually higher concentrations than most other elements.6 7 However, only zinc concentration was correlated with oxidative DNA damage in the electronic cigarette group. While zinc is required for normal human health, its elevation above normal levels has been associated with oxidative stress.40 Our data provide the first evidence that electronic cigarette usage increases the risk of zinc exposure, which in turn causes oxidative DNA damage in humans. Selenium is also a required trace element that can cause harm when elevated.41 While its elevation in electronic cigarette users was not linked to increased oxidative stress, future work may find that it has other adverse health effects.
Oxidative damage can lead to gradual harm of all organ systems42 and if left unchecked can culminate in diseases such as atherosclerosis, coronary heart disease, pulmonary fibrosis, acute lymphoblastic leukaemia and lung cancer.43 Of particular concern, increases in both 8-isoprostane and 8-OHdG were significantly greater in the older populations, suggesting that conventional cigarette users who give up smoking and switched to electronic cigarettes may be at greater risk for oxidative damage than young people who have not smoked previously. In the case of 8-isoprostane, women were more affected than men, suggesting that women should not be encouraged by physicians to use electronic cigarettes, especially when pregnant. There were no significant differences in the elevated concentrations of oxidative harm biomarkers between electronic cigarette users and cigarette smokers, suggesting their organ systems are exposed to similar levels of oxidative damage.
Conclusions
Our data show for the first time that electronic cigarette use, which correlates with metal intake, leads to an elevation in metallothionein in the urine. The usage of electronic cigarettes causes an increase in oxidative stress as measured by 8-OHdG and 8-isoprostane. Electronic cigarette users were exposed to elevated levels of selenium and zinc. The intake of metals (specifically zinc) is further correlated with increased oxidative damage to DNA. These data indicate that electronic cigarette use is not harm free and that prolonged use with elevation of oxidative stress may lead to disease progression. Given these observations, physicians should use caution in recommending the use of electronic cigarettes to their patients and should be alert to possible adverse health outcomes associated with electronic cigarette use. The biomarkers used in this study may be valuable in clinical practice when evaluating the health of electronic cigarette users.
References
Footnotes
Contributors SS-C, MH, MJG and PT were responsible for the study concept and design. SS-C, MW and ANR performed the experiments for data collection. MJG collected and shipped the urine samples to our lab. JL acted as a statistician. SMB helped design the use of the inductively coupled mass spectrometry in TWL’s lab and the analysis of the metal data. SS-C, MW, MH, JL, MJG and PT drafted the manuscript, and all authors read and provided comments on the manuscript. SS-C, MW and PT reviewed the data and take responsibility for the integrity and accuracy of the data. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. SS-C and PT are the guarantors.
Funding This study was supported by the National Institute on Drug Abuse and the National Cancer Institute of the National Institutes of Health (awards R01DA037446 and P30 CA016056, respectively) and FDA Center for Tobacco Products and by an award from the Roswell Park Alliance Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies. MJG reports grants from Pfizer (2011 GRAND [Global Research Awards for Nicotine Dependence] recipient) and personal fees from Johnson & Johnson (as a member of the advisory board) outside the submitted work.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by Roswell Park Comprehensive Cancer Center IRB (protocol number I 247313). The biomarker measurement study was approved under IRB protocol HS-12-023 from University of California, Riverside.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All relevant data are in the manuscript.