Article Text

Abstract
We performed a systematic review of the current state of the literature regarding the natural history and outcomes of bicuspid aortic valve (BAV). PubMed and the reference lists of the included articles were searched for relevant studies reporting on longitudinal follow-up of BAV cohorts (mean follow-up ≥2 years). Studies limited to patients undergoing surgical interventions were excluded. 13 studies (11 502 patients with 2–16 years of follow-up) met the inclusion criteria. There was a bimodal age distribution (30–40 vs ≥50 years), with a 3:1 male to female ratio. Complications included moderate to severe aortic regurgitation (prevalence 13%–30%), moderate to severe aortic stenosis (12%–37%), infective endocarditis (2%–5%) and aortic dilatation (20%–40%). Aortic dissection or rupture was rare, occurring in 38 patients (0.4%, 27/6446 in native BAV and 11/2232 in post). With current aggressive surveillance and prophylactic surgical interventions, survival in three out of four studies was similar to that of a matched general population. In this systematic review, valvular dysfunction warranting surgical intervention in patients with BAV were common, aortic dissection was rare and, with the current management approach, survival was similar to that of the general population.
- Bicuspid aortic valve
- outcomes
- review
Statistics from Altmetric.com
Introduction
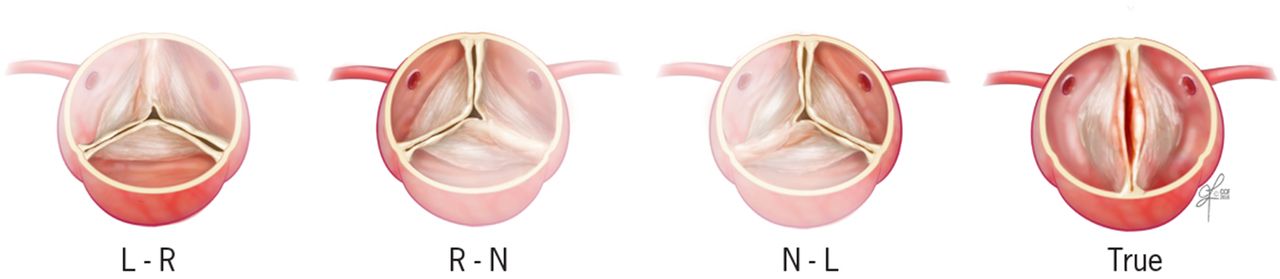
Bicuspid aortic valve (BAV) is a common cardiac anomaly that affects 0.5%–2% of adults.1 BAV is a part of a syndrome with various phenotypes that includes true bicuspid or three cusps with fusion of two out of three cusps (figure 1).2 It has a variable course ranging from asymptomatic status, isolated aortic valve regurgitation (AR) or aortic stenosis (AS), infective endocarditis (IE), aortic dilatation or a combination of these (figure 2). There are no well-established trials or longitudinal registries of patients with BAV, and most studies are observational and retrospective in nature. The purpose of this review is to systematically evaluate the natural history and management of BAV as reported in longitudinal studies.
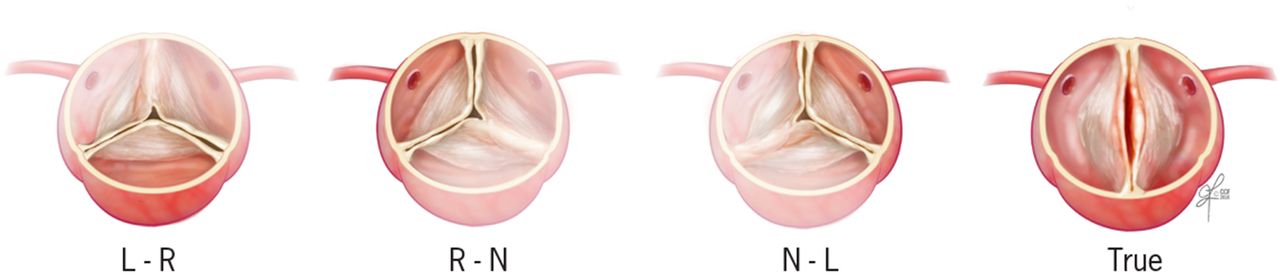
Schematic illustration of a bicuspid aortic valve as a true bicuspid versus a trileaflet valve and fusion of two out of three cusps (L-R suggesting fusion of left and right cusps, R-N suggesting fusion of right and non-coronary cusps and N-L suggesting fusion of left and non-coronary cusps).

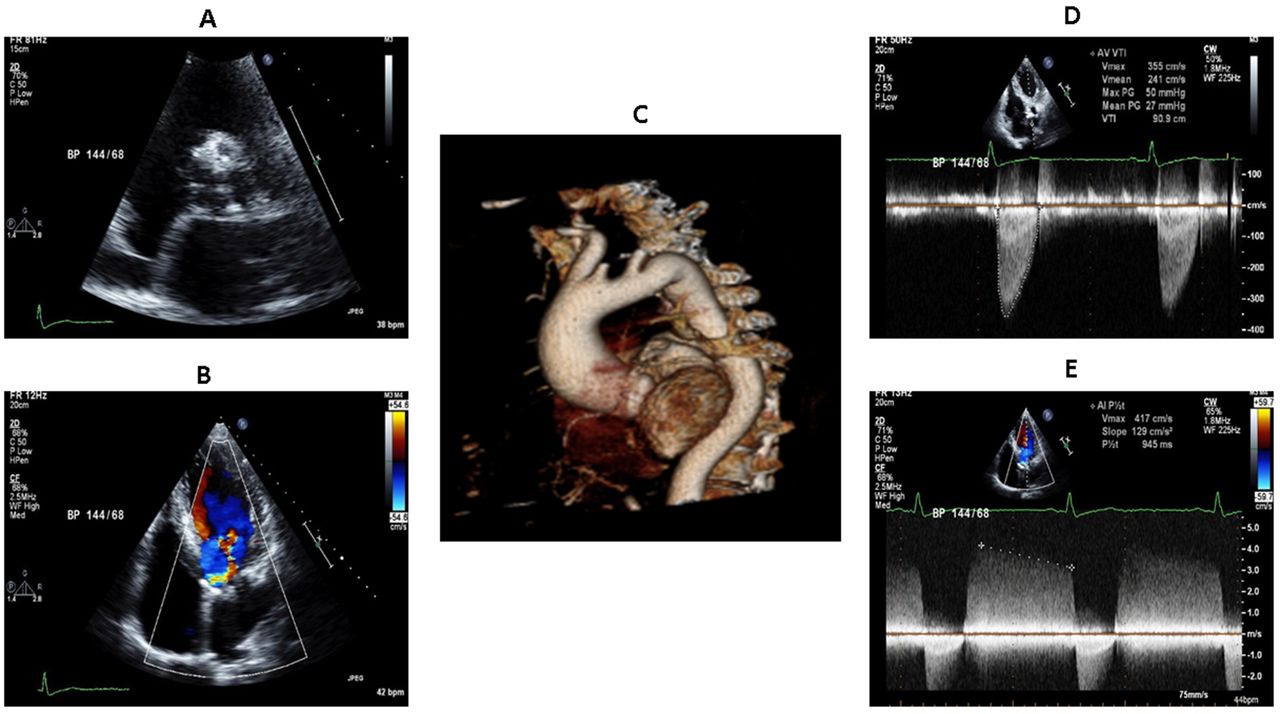
Multimodality imaging in a 53-year-old man with bicuspid aortic valve (BAV) and concomitant aortopathy. (A) Short axis view on two-dimensional transthoracic echocardiography demonstrating a heavily calcified BAV. (B) Four-chamber view on two-dimensional transthoracic echocardiography with colour Doppler demonstrating moderate aortic regurgitation. (C) Volume rendered contrast-enhanced gated CT scan of the thoracic aorta demonstrating aneurysmal dilation of the ascending aorta. (D) Spectral Doppler demonstrating moderate aortic stenosis. (E) Spectral Doppler demonstrating moderate aortic regurgitation.
Methods
We conducted this systematic review in accordance with the preferred reporting items for systematic reviews and meta-analyses guidelines.3 PubMed was searched for studies published from 1990 to January 2017 (figure 3). Search terms included ‘bicuspid aortic valve’, ‘bicuspid aortopathy’, ‘bicuspid natural history’, ‘bicuspid complication’, ‘bicuspid survival’, ‘bicuspid surgery’, ‘bicuspid dissection’ and ‘non-syndromic aortic dissection’. Subsequently, a manual search of the reference lists of selected articles was done. Our search was limited to studies in English language, reporting on the natural history of BAV and/or BAV-related aortopathy with longitudinal follow-up ≥2 years. We excluded studies reporting on patients presenting prior to 1980 and those reporting only on patients undergoing surgical interventions. We included surgical studies that followed up patients post-AVR (aortic valve replacement) to study the natural history of aortic complications. Full texts of potential studies were reviewed. Given the few publications on this subject, we included manuscripts from the same institution if they provided added value over the most comprehensive and detailed publication. Bias was assessed using the modified Newcastle-Ottawa Scale for non-randomised studies.4 Relevant study characteristics were collected from individual studies. Outcomes of interest were AVR, aorta-related surgeries, all-cause mortality and cardiac mortality when reported. Complications were defined as the development of AS, AR, IE, aortic aneurysm and aortic dissection. Given the significant methodological differences among the included studies, a meta-analysis was not done.

Preferred reporting items for systematic reviews and meta-analyses flow diagram for search strategy and results.
Results
We identified 13 studies that were included in this systematic review (figure 3). All the included studies are summarised in table 1. The Michelena et al 2011 study5 included all the patients from the Michelena et al 2008 study,6 but, given the incremental information provided by the Michelena et al 2008 study (where only asymptomatic patients were included and followed up), both studies were included in this review. However, to avoid double-counting patients, the Michelena et al 2008 study was not included in the overall number of patients reported in this review.
Characteristics of the studies included in the systematic review (n=13)
Natural history and demographics
Relatively few studies have attempted to answer the question of natural history of BAV and its complications; 13 studies are included in this review (table 1). Studies were of two categories: those evaluating all outcomes in a defined cohort of patients with BAV5 7–14 and those that specifically evaluated aortic complications in a prespecified subgroup of patients with BAV.15–17 All studies were observational.5–17 The majority of the studies had a mean age between 30 and 40 years,5–7 9 11 13 whereas some had mean age ≥45 years.8 12 15 17 This has significant implications when evaluating the outcomes in these patients, given that older patients are expected to encounter more interventions and generally have worse outcomes. AR was the most common underlying complication in younger patients, whereas AS and aortopathy were usually present later in life.7 There was a male predominance with a male to female ratio of 3:1.5–10 12–17 In one study that reported on gender-specific outcomes for patients undergoing AVR (thus not included in data synthesis), women were older, had less AR and had more comorbidities with a higher operative risk, but short-term and long-term outcomes were similar to that of men.18 Similarly, Michelena et al showed similar long-term survival in both genders, but women had higher risk of death in the clinical and surgical tertiary referral settings, whereas men had worse BAV-related morbidity in the community settings.14
Many other lesions and syndromes are associated with BAV, including aortic coarctation and patent ductus arteriosus. Coarctation-mediated hypertension greatly increased the risk of aortic dissection.19 In the presurgical era, death from aortic dissection occurred in 19% of patients with BAV and in 50% of patients with concomitant BAV disease and coarctation.2 20 However, while surgeries could be life saving, these numbers could be an overestimate, reflecting selection biases in earlier studies. Aortic coarctation accompanies BAV much more commonly in men (4:1) than in women.
BAV morphology and natural history
It remains controversial whether BAV morphotype (ie, patterns of cusp fusion) can predict the progression of aortic valve (AV) dysfunction or the development of aortic aneurysms.21 22 However, a recent study evaluated the prognostic implications of raphe in 1881 patients with BAV compared with 237 patients with BAV without raphe.12 This study showed that the presence of a raphe was associated with a higher prevalence of significant AS, AR and need for AVR, but it was not an independent predictor of all-cause mortality.
Clinical presentation
Asymptomatic
Eight studies evaluated outcomes of 8205 patients with BAV over a follow-up period ranging from 2 to 16 years generally without restricting the inclusion criteria to aortic complications of BAV or subsequent to AVR.5–9 11–14 While it is hard to evaluate the prevalence of truly asymptomatic patients with BAV, studies used need for intervention, dissection and mortality as indirect measures of ‘symptoms’. The caveat is some patients did not have symptoms but underwent surgical intervention based on either their own preference or that of the treating cardiologist. In the only study that included patients without apparent complications at inception (n=212), almost half of the patients (42%) had either a medical or a surgical event at 15 years of follow-up.6
Aortic regurgitation
AR is highly prevalent in patients with BAV, ranging between 47% and 64%.5 6 8 12 13 16 However, moderate to severe AR with or without ventricular dysfunction is more reflective of the prevalence of a ‘complication’ because this would directly affect patients’ outcomes and lead to surgical intervention. Few studies have reported on moderate to severe AR prevalence in BAV,6–8 12–14 but those showed a varied prevalence between 13% and 32%, probably representing community cohorts versus referral bias in the tertiary care settings. AR tends to present at a younger age when compared with AS, with a mean age around 45 years (vs 54 years for significant AS).8 In a recent study of 1417 mostly asymptomatic patients (37% with BAV) with ≥III+ AR, there was significantly improved long-term survival following AV surgery, similar to that of an age-matched and gender-matched population.23
Aortic stenosis
In adults, BAV typically presents in the fifth or sixth decade. Progression of stenosis is probably similar to that of trileaflet AV (TAV) stenosis but is manifested at least 5–10 years earlier in patients with BAV.24 The natural history of AS and progression of stenosis severity are all derived from cohorts defined as having AS without necessarily defining the underlying valve morphology.25–27 While it is plausible that the rate of progression of AV stenosis is faster in BAV when compared with TAV and hence patients’ present at an earlier age, currently there are no studies that specifically address the rate of progression of AS in BAV. The included BAV studies showed that 12%–37% patients had or developed moderate to severe AS.7 8 12–14 One study, which included patients with no complications related to BAV at baseline, showed that over 15 years of follow-up, 26 out of 212 patients with BAV (12.3%) underwent surgical AVR for severe AS.6 Another study showed that the majority of surgical referrals in BAV were secondary to symptomatic AS.7
Mixed AS and AR
Limited data exist on the natural history and outcomes of patients with mixed AS and AR, as it is not commonly encountered in patients with BAV. Significant mixed AS and AR developed only in 1% of the patients in the study by Michelena et al 6 and was present in 3% of the patients in the study by Masri et al.8 Another recent study evaluated the outcomes of 251 patients with mixed moderate AS and AR, of which 38% had BAV.28 The study showed that the rates of adverse outcomes in this group were similar to that of an age-matched and sex-matched cohort with severe AS, and much worse than the rates with isolated moderate AS or moderate AR.28 This warrants further study to evaluate the natural history of mixed AR and AS in BAV and whether it warrants earlier surgical intervention.
Infective endocarditis
IE rates were thought to be high in patients with BAV warranting antibiotic prophylaxis based on older studies.29 In three previous cohorts, the incidence of native valve IE in BAV has been reported to be 2%–2.5%.6–8 A recent community-based report showed native BAV IE incidence of 9.9 per 10 000 patient-years.30 Two recent studies which followed patients up to 2015 showed a higher incidence of 3.7%–5%.12 13 The majority of these patients were followed in the pre-2007 or antibiotics era, which could have masked the actual incidence. Hence, the actual incidence of IE in patients with BAV in the era of no antibiotic prophylaxis is yet to be determined, especially in light of the higher incidence reported in the two recent studies.12 13
Aortopathy
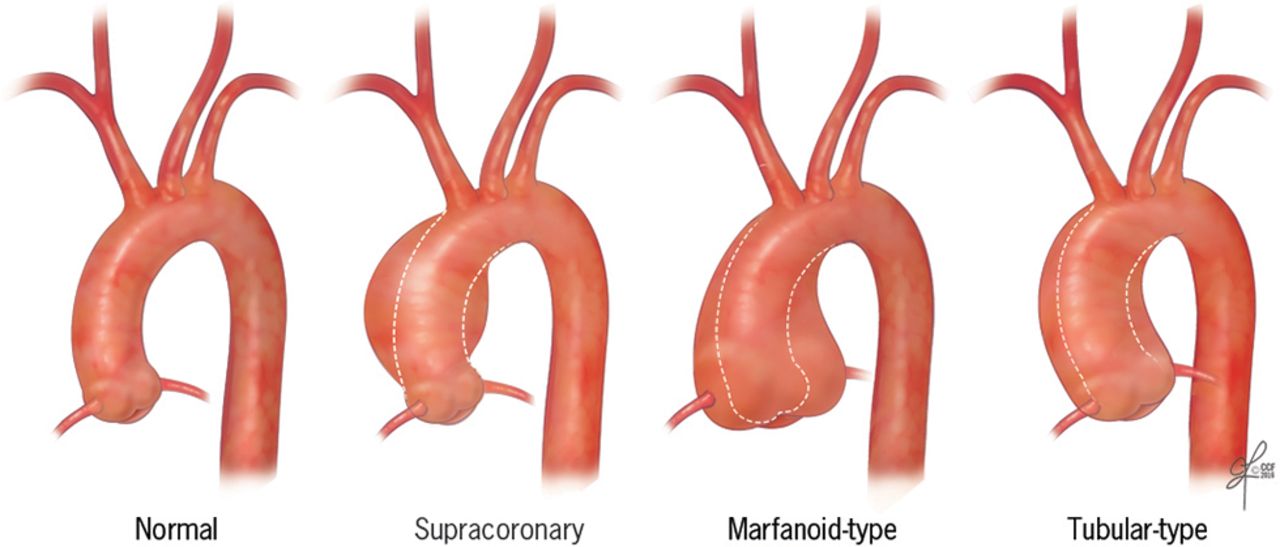
BAV-associated aortopathy has a prevalence of 40% of patients in referral centres8 (figure 4). Dilation may occur in the aortic root, the tubular ascending aorta, the proximal aortic arch or any contiguous combination of these three.31 Two studies reported an incidence of 20% of aortic aneurysms over 9–16 years of follow-up.5 7

Schematic illustration of different aortic dilation patterns noted in patients with bicuspid aortic valve.
Many studies have evaluated the aortic complications of BAV including aortic dilatation, aneurysm, dissection, rupture and death (table 1). This is generally reported apart from surgical intervention for coexisting coarctation, which was present generally in 1%–7% of patients,5–8 14 15 except for the studies by Tzemos et al (25%)7 and Rodrigues et al (18.9%).13 Current guidelines emphasise routine surveillance and early elective surgical intervention, beyond specific aortic diameter thresholds.32 33
Despite being heterogeneous, natural history studies have shown the low incidence of aortic dissection (table 1). These studies were heterogeneous in the definition of aortic aneurysm (a maximal aortic diameter cut-off of 35, 40 and 45 mm), the exact segment of the aorta that was dilated (root vs ascending vs arch vs descending aorta) and the method used for diagnosis and follow-up (mostly transthoracic echocardiogram, with many studies having patients in the era prior to tomographic imaging evaluation). Aortic dilatation was present in 20%–42% of the patients (table 1). In the study by Michelena et al, 32 patients (7.7%) had dilated aorta (defined as aorta ≥45 mm). Over 16 years of follow-up, 49 patients (12.7%) developed dilated aorta, 2 suffered from aortic dissection (1 type A, 1 type B; 25-year cohort risk of dissection was 0.5%) and 49 patients (11.7%) underwent surgery related to the aorta.5 In a prior publication involving the same cohort, where only asymptomatic patients at baseline were included, 15% of the patients had aortic dilatation at baseline, and this fraction increased to 39% over 15 years of follow-up, with no dissection or death due to aortic complications reported, but eight patients underwent surgery for aortic aneurysm.6 In the study by Tzemos et al, 10% of the patients had dilated aorta (≥40 mm) at baseline. Over 9 years of follow-up, five patients (0.7%) suffered dissections (three ascending, two descending), 6.7% of the patients underwent surgery related to the aorta and 20% had dilated aorta.7 In the study by Masri et al, 42% of the patients had dilated aorta ≥40 mm, with only 2 (0.1%) confirmed dissections occurring over 8.1 years of follow-up.8 In the GenTAC registry, out of 770 patients with no aortic aneurysm at baseline, 2 patients suffered aortic dissection over 3.6 years of follow-up. Sherrah et al reported on 225 patients with BAV with an initial proximal aortic diameter of 44.1±8.4 mm. Over a median of 7 years, there were zero dissections.9 Rodrigues et al reported on 227 patients with only two dissections (1%) occurring over 13±9 years. In a large international registry of 2118 patients with BAV treated at tertiary referral centres, there were eight dissections (0.4%) over a median of 2 years. Only one study by Davies et al showed a high rate of dissection (six patients or 8.5% over 5.4 years of follow-up); however, all included patients had a dilated aorta (≥35 mm), 57.1% had an aortic diameter ≥45 mm and 10% had an aortic diameter ≥55 mm at baseline, making such findings not applicable to the general BAV population.34 The question of adverse aortic outcomes in patients with a replaced BAV was evaluated by two studies.15 17 In the first study, Girdauskas et al evaluated 153 patients with BAV who underwent AVR for AS, where 39% of the patients had an aortic diameter ≥45 mm. Over 11.5 years, there were zero dissections and five patients (3%) underwent surgery related to the aorta. In the second study, Itagaki et al evaluated 2079 patients with BAV and reported aortic dissection incidence of 0.55% at 15 years.15
Overall, these studies confirmed that the most serious complication associated with BAV (ie, dissection) was rare; 36 dissections and two aortic ruptures out of 8678 patients with BAV and an incidence rate of 0.4% over a follow-up period of 2–16 years (27/6446 in native BAV and 11/2232 in post-AVR).5–17 The limitation is that it would be impossible to know whether this is secondary to the actual low incidence of dissection in patients with BAV or just a reflection of the active surveillance and elective surgical intervention. In all of the reported studies in this review, only six patients had their aortic dimension known prior to dissection, and five of them had a maximal thoracic aortic diameter of ≤55 mm .5 8 10 Although the American College of Cardiology/American Heart Association guidelines’ recommendations would not necessarily have advocated elective aortic surgery in these patients, all the referenced outcomes in this review provide reassurance that the current practice is safe and dissection in BAV is uncommon.
BAV in pregnancy
The frequency of cardiovascular events in pregnant women with BAV was evaluated in 88 women with a mean age of 35 years, with a total of 216 pregnancies and 186 deliveries.11 There was no association between pregnancy and aortic dissection, aortic surgery or AVR. This is probably related to the low incidence of aortic dilatation/aneurysm, as only one patient had an aorta >50 mm at the time of diagnosis, and after 10.7 years of follow-up, only two patients had aortas >50 mm. However, this study did confirm that the rate of progression of aortic dilatation is significant, as only 5 patients (6%) had aortas >40 mm at diagnosis, but this number increased to 21 patients (35%) after 10.7 years of follow-up.11
Mortality
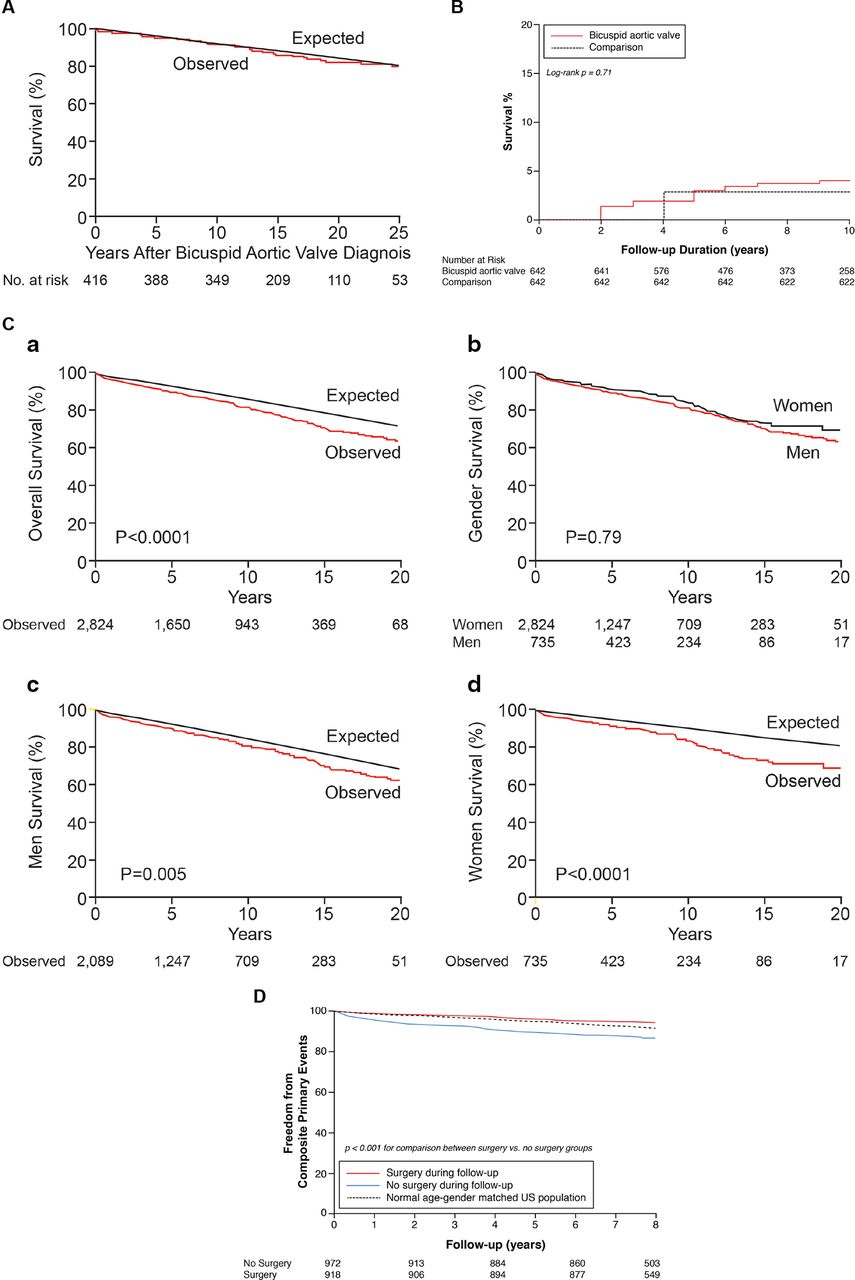
Death in patients with BAV can be secondary to aortic complications (dissection or rupture) or secondary to progressive AV dysfunction or endocarditis. When examining data obtained from retrospective and natural history studies, it is important to include patients suffering from sudden, unexplained cardiac death as cases of presumed aortic complications. With the current aggressive surveillance and prophylactic surgical interventions, the ultimate goal of treating patients with BAV is to improve survival. In two cohorts that enrolled patients over a long time period (1980–2001) with a mean age range of 32–35 years, survival was similar to that of age-matched and sex-matched general population5–7 (figure 5A,B). In a recent study of 2824 patients with BAV referred to a tertiary centre and followed up for 9±6 years, survival was worse when compared with age-matched and sex-matched population (64% vs 72%, p<0.0001), with no statistically significant difference in survival in men versus women (62% vs 70%, p=0.79) (figure 5C).14 In a more contemporary cohort referred to a tertiary centre between 2003 and 2007, survival of patients with BAV who underwent surgery related to BAV was similar to that of the matched general population, but better than patients with BAV who did not undergo BAV-related surgeries8 (figure 5D). However, there were a few key differences in the two cohorts, including a higher mean age (62 vs 51 years) and a higher proportion of patients in New York Heart Association class III/IV (50% vs 5%) in the Michelena et al 14 versus the Masri et al 8 cohort. However, further investigation is needed to compare the outcomes of patients with BAV who undergo BAV-related surgery compared with those who do not, as well as establishing a more precise way of selecting patients for prophylactic aortic surgery.
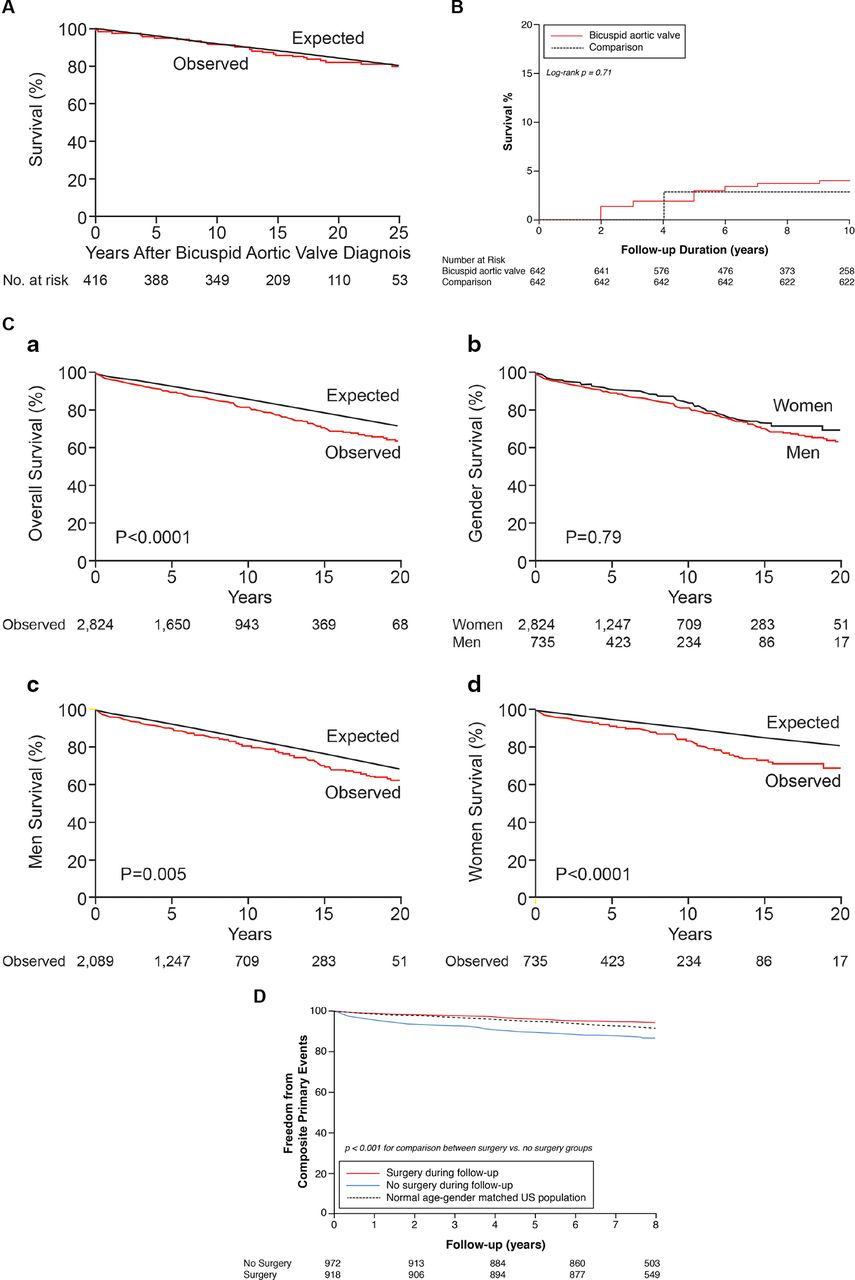
Survival curves of different bicuspid aortic valve (BAV) cohorts compared with age-matched and gender-matched normal population: (A) community-based cohort with BAV (adapted with permission from Michelena et al 5 ), (B) adults with BAV (adapted with permission from Tzemos et al 7 ), (C) tertiary referral centre cohort from 1990 to 2011 (adapted from Michelena et al 14) and (D) contemporary cohort with BAV from 2003 to 2007 (adapted with permission from Masri et al 8).
Surgical management of BAV and survival
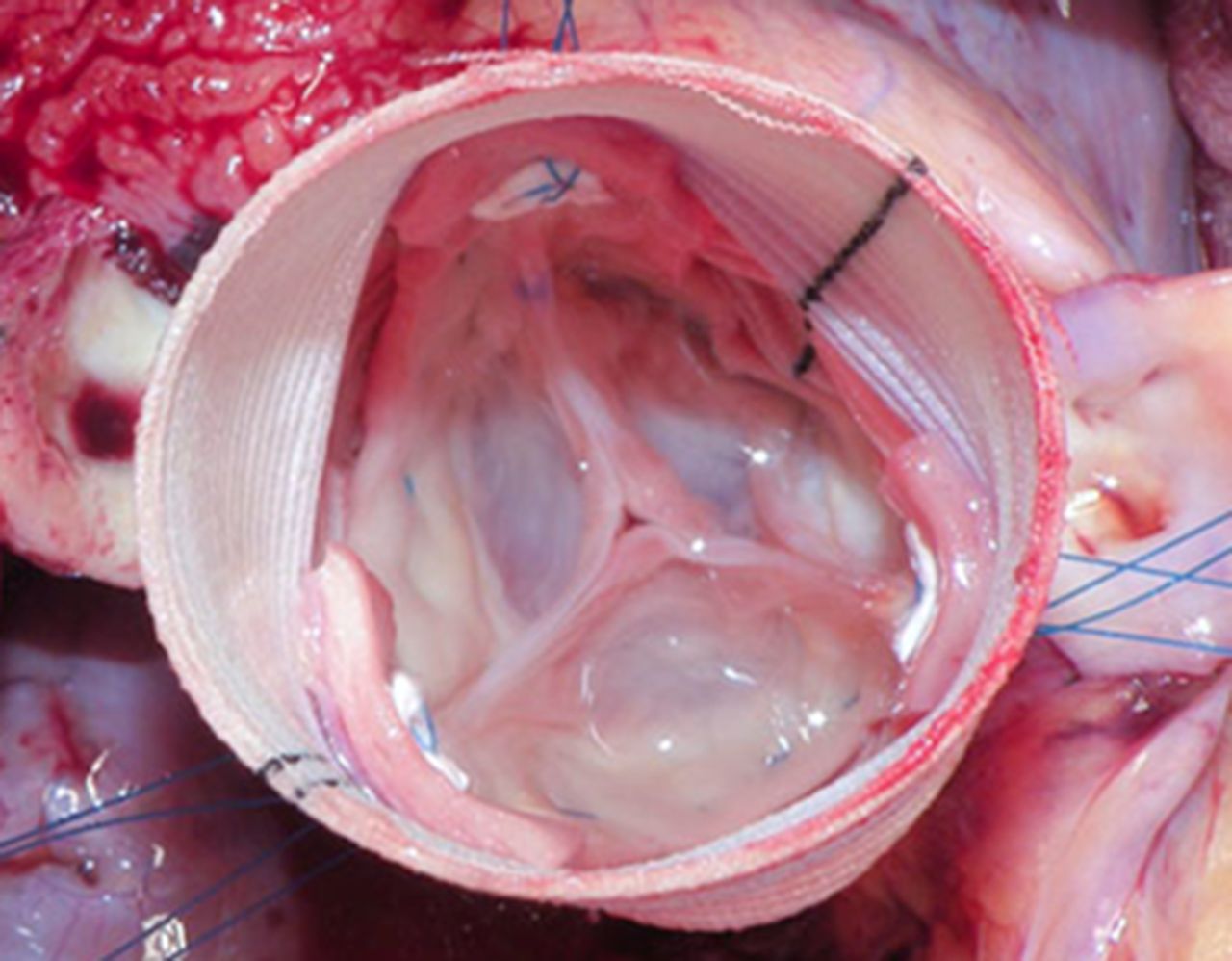
AV dysfunction resulting in AV repair or replacement (figure 6) is the most common complication of BAV, ranging from 16% to 68% of included patients (table 1).5–17 Including the studies that evaluated all comers with BAV, 2326 patients (28%) underwent AV repair or replacement (the most common indication being AS as opposed to regurgitation). However, BAV is a complex disease with multiple potential associated conditions that may require concomitant surgical intervention (including valve-sparing root replacement, figure 7), as illustrated in a recent series, where out of 918 patients (49%) undergoing BAV-related surgical intervention only 332 patients (36%) had isolated AV surgery and 30 patients (3.3%) had isolated aortic grafting.8 It has also been shown that for a young asymptomatic population with BAV, the rate of surgical events at 16 years was 27%.6 However, the mean age in that study was 32 years.6 When evaluating mortality for patients who underwent surgery versus those who did not, we showed that surgery led to a 56% relative risk reduction of all-cause mortality and dissection.8
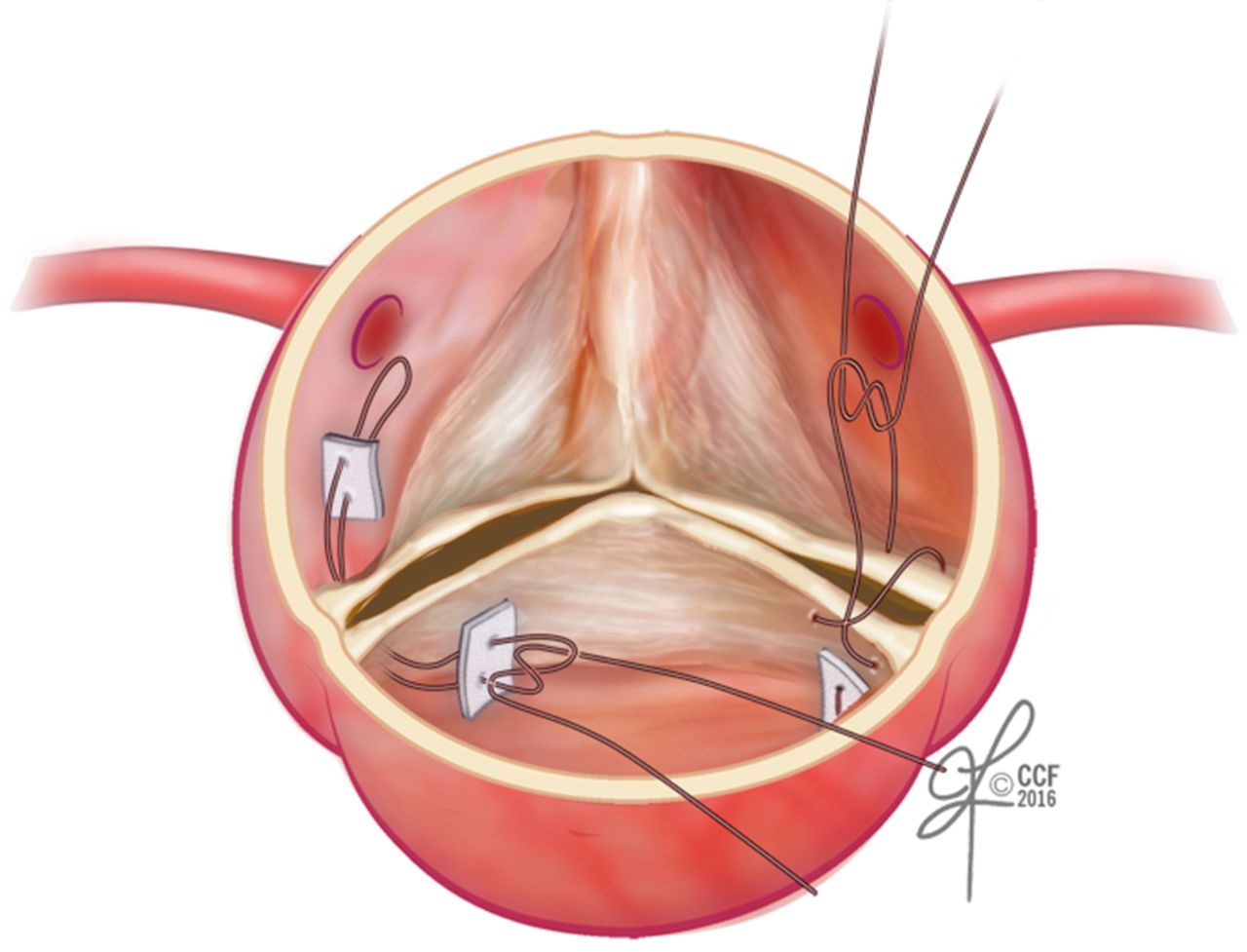
Schematic illustration of a standard aortic valve repair technique.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Image of a valve-sparing aortic root replacement.
Conclusion
BAV is a common cardiac anomaly associated with significant medical and surgical morbidity over the life of affected individuals. Studies evaluating the natural history of BAV are reassuring in reporting a consistently low incidence of dissection and mortality probably similar to that of the general population. As these studies were conducted in the era of aggressive surveillance and prophylactic surgical interventions, continuous evaluation of the outcomes in patients with BAV is required in parallel with the change in the guidelines. A long-term, contemporary, prospective and longitudinal community-based study is needed to further characterise the natural history of BAV in the current era of evidence-based medicine.
Acknowledgments
Dr Svensson acknowledges the David Whitmire Hearst Jr Foundation for supporting aortopathy research at the Cleveland Clinic. Dr Griffin is supported by the Brown family endowed chair in cardiovascular medicine. Dr Desai is supported by the Haslam family endowed chair in cardiovascular medicine.
References
Footnotes
Contributors AM, BPG, LGS and MYD worked on the draft and revisions and take full responsibility for the paper.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.