Article Text

Abstract
Background Neisseria gonorrhoeae has developed resistance to most antimicrobials used for treatment. Worryingly, treatment failures with oral extended-spectrum cephalosporins (ESCs) have been reported, especially in the WHO Western Pacific Region, and susceptibility to all ESCs (oral and injectable), the last remaining treatment options in many settings, is decreasing globally.
Objectives To examine the emergence, spread and characteristics of Neisseria gonorrhoeae isolates with decreased susceptibility and resistance to ESCs in Sweden.
Methods All available Swedish isolates from 1998–2009, collected from many countries worldwide, displaying decreased susceptibility to cefixime and/or ceftriaxone (minimum inhibitory concentration (MIC) ≥0.032 mg/l; n=331) were examined using antibiograms, full-length porB gene sequencing, N gonorrhoeae multi-antigen sequence typing (NG-MAST), and sequencing of ESC resistance determinants (penA, mtrR and porB1b (penB alteration)).
Results Based on EUCAST breakpoints, 30 (9.1%) and one (0.3%) of the isolates displayed in vitro resistance to cefixime and ceftriaxone, respectively. penA mosaic alleles and penA A501 alteration were detected in 24% and 11%, respectively, of the isolates, and in increasing prevalence over the years. Moreover, among these isolates 38 NG-MAST sequence type (STs) were detected, with ST1407 (n=29), ST1103 (n=9) and ST3378 (n=8) being most common.
Conclusions The proportions of N gonorrhoeae isolates with decreased susceptibility and resistance to ESCs have substantially increased over the years in Sweden. Both penA mosaic alleles and the penA A501 alteration, together with mtrR and penB, are important for the decreased susceptibility and resistance to ESCs. At least one gonococcal penA mosaic strain (ST1407), including its evolving subtypes, with decreased susceptibility/resistance to ESCs circulates worldwide.
- Neisseria gonorrhoeae
- antimicrobial resistance (AMR)
- ceftriaxone
- cefixime
- penA mosaic allele
- gonococci
- gonorrhoea
- STD
- surveillance
Statistics from Altmetric.com
- Neisseria gonorrhoeae
- antimicrobial resistance (AMR)
- ceftriaxone
- cefixime
- penA mosaic allele
- gonococci
- gonorrhoea
- STD
- surveillance
Neisseria gonorrhoeae is the aetiological agent of gonorrhoea, which remains a global public health problem. Most worryingly, N gonorrhoeae has developed high-level resistance to all antimicrobials used in the traditional treatment of gonorrhoea, for example penicillins, tetracyclines and fluoroquinolones.1 Furthermore, in recent years gonococcal strains with resistance and/or decreased susceptibility to azithromycin, including high-level resistance, and the currently ideal treatment options extended-spectrum cephalosporins (ESCs), have emerged.1–10 Treatment failures using oral ESCs including cefixime are occurring, especially in the WHO Western Pacific Region (WPR),1 5 11–13 and susceptibility to all ESCs (oral and injectable) is decreasing globally. However, verified failures of treatment for urogenital gonorrhoea using ceftriaxone (injectable) are still lacking. Nevertheless, the emergence and spread of decreased susceptibility and resistance to ESCs are serious concerns globally and gonorrhoea may become untreatable in certain circumstances.
The first molecular mechanism for decreased in vitro susceptibility and resistance to ESCs is alteration of the penA gene, that is acquisition of a penA mosaic allele that encodes an altered penicillin binding-protein 2 (PBP2).1 3–10 13–15 However, alterations of a single amino acid, that is A501, of PBP2 in non-mosaic penA alleles may also decrease ESC susceptibility.1 4 6 16 Furthermore, mutations in the promoter and/or coding sequence of the repressor gene mtrR, which cause over-expression of the MtrCDE efflux pump system, further decrease ESC susceptibility.1 3 5 15 17 In addition, specific porB1b gene mutations (the penB resistance determinant) that alter amino acid G101 and A102 in the outer membrane PorB1b porin result in decreased permeability and thus further decreased susceptibility to ESCs.1 3 5 15 18 19 Finally, at least one unknown resistance determinant exists,3 15 and accordingly the mechanisms that underlie the development of ESC decreased susceptibility and resistance are not yet all known.
Most, if not all, resistance in N gonorrhoeae to different antimicrobials has historically emerged in the WHO WPR. This resistance has subsequently and rapidly been spread worldwide by sex tourists and other travellers.1 The emergence and spread of ESC decreased susceptibility and resistance globally will most probably follow the same pattern. Accordingly, in 2001 two cases of treatment failure with oral cephalosporins had already been reported in Japan,20 and in 2006 all oral ESCs were excluded from the treatment guidelines for gonorrhoea in Japan, due to the high level of resistance.1 5 In Sweden, the first gonococcal isolate with decreased susceptibility to ESCs, which also contained the characteristic penA mosaic allele X10 and was indistinguishable from the Japanese isolates causing treatment failures, was found in 2002.3
The aims of this study were to examine the emergence, spread, and phenotypic as well as genotypic characteristics of N gonorrhoeae isolates with decreased susceptibility and resistance to ESCs in Sweden.
Methods
N gonorrhoeae isolates
All examined isolates were obtained by the National Reference Laboratory for Pathogenic Neisseria, Örebro University Hospital, Sweden from 1998 through 2009. All N gonorrhoeae clinical isolates displaying a minimum inhibitory concentration (MIC) of ≥0.032 to cefixime and/or ceftriaxone were included (n=331). These isolates were from 331 patients (18% females and 82% males). The mean age of the males was 34 years (median age 31 years, range 16–68 years) and the mean age of the females was 34 years (median age 32 years, range 15–59 years). Gender distribution and age distribution were relatively similar during the years examined. Unfortunately, complete data regarding the sexual orientation of the patients and the country of exposure to infection were not available. However, data available showed that patients included both heterosexuals and men who have sex with men (MSM). Furthermore, heterosexuals in particular were exposed to the infection in many countries worldwide (eg, European countries (n=14, spread all over Europe), African countries (n=3), Asian countries (n=6), Australia and the USA). The isolates were species confirmed with a sugar utilisation test and/or the Phadebact GC Monoclonal Test (Boule Diagnostics AB, Huddinge, Sweden), and preserved as previously described.21 The WHO 2008 N gonorrhoeae reference strains were included as control strains.22
Antimicrobial susceptibility testing
Susceptibility (mg/l) to cefixime, ceftriaxone, ampicillin, azithromycin, ciprofloxacin and spectinomycin was determined using the Etest method (AB Biodisk, Solna, Sweden), as previously described.23 The breakpoints used for susceptibility (S) and resistance (R) were as follows (according to The European Committee on Antimicrobial Susceptibility Testing – EUCAST; http://www.eucast.org): cefixime: S ≤0.125 mg/l, R >0.125 mg/l; the in vitro breakpoint is only tentative due to the lack of appropriate correlates between in vitro findings and clinical outcome; ceftriaxone: S ≤0.125 mg/l, R >0.125 mg/l; the in vitro breakpoint is only tentative due to the lack of appropriate correlates between in vitro findings and clinical outcome; ampicillin: S ≤0.125 mg/l, R >2 mg/l; azithromycin: S ≤0.25 mg/l, R >0.5 mg/l; ciprofloxacin: S ≤0.032 mg/l, R >0.064 mg/l; and spectinomycin: S ≤64 mg/l, R >64 mg/l. β-Lactamase production was detected using nitrocefin discs.
Isolation of genomic DNA
Bacterial DNA was isolated in the robotised NorDiag Bullet instrument (NorDiag ASA, Oslo, Norway) using the BUGS'n BEADS STI-fast kit (NorDiag ASA), according to the manufacturer's instructions.
Detection of penA mosaic alleles and alteration of amino acid A501 in PBP2
All gonococcal isolates (n=331) were screened for the presence of a penA mosaic allele using a previously described penA mosaic allele conventional PCR,24 as well as a previously described method based on real-time PCR and pyrosequencing.25 Both these methods were used in order to identify most/all types of penA mosaic alleles; the pyrosequencing method also identifies alterations of A501 in PBP2. DNA of the WHO 2008 N gonorrhoeae WHO reference strain K,22 which contains the characteristic penA mosaic allele X,10 and sterile water were included in each run as positive control and negative control, respectively.
mtrR and porB1b sequencing
The promoter and coding sequence of mtrR, and the full-length porB1b gene were sequenced in all isolates possessing a penA mosaic allele or any alteration of A501 in PBP2 (n=115), as previously described.3 22 DNA of the WHO 2008 N gonorrhoeae reference strain M22 and sterile water were included in all runs as positive control and negative control, respectively.
N gonorrhoeae multiantigen sequence typing (NG-MAST)
NG-MAST was performed on all isolates possessing a penA mosaic allele or any alteration of A501 in PBP2 (n=115), as previously described.26 NG-MAST allele numbers of porB and tbpB, and sequence types (STs) were assigned using the NG-MAST database (http://www.ng-mast.net).
Sequence alignments and phylogenetic analysis
Multiple-sequence alignments of nucleotide sequences and the deduced corresponding amino acid sequences were performed in the software BioEdit Sequence Alignment Editor v 7.0.9.0 with manual adjustment.
Phylogenetic analysis of the full-length porB1b gene encoding the mature PorB1b was performed with the software TREECON (v 1.3b) by using the Jin and Nei substitution model, the Kimura evolutionary model, an α value of 0.5 and the neighbour-joining method, as previously described.26
Results
Longitudinal trends in the MICs of cefixime and ceftriaxone
The distributions of MICs of cefixime (2003, which was the first year all isolates were examined, and 2009) and ceftriaxone (1998 and 2009) displayed distinct shifts towards higher MICs over the years for both antimicrobials. Increased proportions of isolates with MICs above the tentative in vitro resistance breakpoints, cefixime 5.2% (n=12) in 2009 and ceftriaxone 0.4% (n=1) in 2009, were identified (figure 1).

Distribution of Neisseria gonorrhoeae minimum inhibitory concentrations (MICs) of (A) ceftriaxone (1998 and 2009) and (B) cefixime (2003, which was the first year all isolates were examined, and 2009). The tentative in vitro breakpoints for resistance (http://www.eucast.org) are indicated as a dashed line. 1998, 348 isolates; 2003, 130 isolates; and 2009, 230 isolates.
Antimicrobial susceptibility of all selected N gonorrhoeae isolates from 1998 to 2009 (n=331)
Based on the EUCAST breakpoints, 30 (9.1%) of the strains displayed in vitro resistance to cefixime. However, 330 (99.7%) of the isolates were susceptible to ceftriaxone, and accordingly only one isolate showed resistance (MIC=0.250 mg/l). Among all the isolates, 8% were resistant to ampicillin, 17% to azithromycin, and 91% to ciprofloxacin; however, no isolates resistant to spectinomycin were found. β-Lactamase production was identified in 41 (12%) of the isolates.
The year of collection, number of isolates, presence of ESC resistance determinants, and susceptibility to ESCs of all isolates are summarised in table 1.
Neisseria gonorrhoeae displaying increased MICs of cefixime and/or ceftriaxone (≥0.032 mg/l) isolated in Sweden (n=331), 1998–2009
penA mosaic allele and alteration of A501 in PBP2
Seventy-eight (24%) isolates contained a penA mosaic allele, identified using the conventional PCR (n=77) and the pyrosequencing method (n=78), and 37 (11%) isolates had an alteration of A501 (A501V, n=33 and A501T, n=4) in PBP2 (tables 1 and 2). However, no isolates contained a penA mosaic allele including any mutations causing an alteration of A501 in PBP2.
The NG-MAST sequence types, year of isolation and MICs of cefixime and ceftriaxone for all Neisseria gonorrhoeae with a penA mosaic allele (n=78) or an alteration of A501 in PBP2 (n=37) isolated in Sweden, 2002–2009
The proportion of isolates with a penA mosaic allele substantially increased from the year 2006 (0.5%) to 2009 (8.1%), while there were no isolates with penA mosaic alleles in 1998–2001, 2004 or 2005. By 2003 there were already 11 isolates with a penA mosaic allele (n=6 in 2002, and n=5 in 2003); however, eight of those had been received from the USA (n=5) and the UK (n=3) for a specific study regarding ESC decreased susceptibility. The prevalence of isolates with PBP2 A501 alteration ranged from 0.7% to 2.3% between 2003, when these were first detected, and 2009. The MICs of cefixime and ceftriaxone for the penA mosaic allele isolates ranged from 0.023 to 0.500 mg/l (mean MIC: 0.064 mg/l) and from 0.008 to 0.250 mg/l (mean MIC: 0.047), respectively. The MICs of the isolates with PBP2 A501 alteration ranged from 0.016 to 0.19 mg/l (cefixime, mean MIC: 0.064 mg/l) and from 0.023 to 0.125 mg/l (ceftriaxone, mean MIC: 0.094 mg/l) (tables 1 and 2). The majority of isolates, 62 (80%) out of 79, that displayed an increased MIC (>0.032) to both cefixime and ceftriaxone, also possessed either a penA mosaic allele or an alteration of A501 in PBP2.
Specific mutations in mtrR and porB1b (penB alteration)
Mutations in the promoter region or coding sequence of the mtrR gene that cause over-expression of the MtrCDE efflux pump were observed in 110 (96%) of the isolates examined (n=115). Ninety-three (81%) had the characteristic single nucleotide (A) deletion in the inverted repeat of the promoter region and eight isolates (7%) displayed alterations of amino acid G45 in MtrR (table 1). Nine (8%) of the isolates contained both these alterations. penB alterations in amino acid 101 and/or 102 were detected in 113 (98%) of the isolates. One of these isolates lacked the alteration in amino acid position 101 and two isolates did not have the alteration in 102. In only five (4%) of the isolates was there a mutation in mtrR in the absence of the penB alteration. All 31 isolates displaying in vitro resistance to cefixime (n=30) and ceftriaxone (n=1) according to EUCAST breakpoints contained penA alterations (mosaic allele, n=30 and A501, n=1) and penB alteration, and 30 of these isolates also contained the single nucleotide (A) deletion in the promoter region of mtrR.
N gonorrhoeae multiantigen sequence typing and phylogenetic analysis
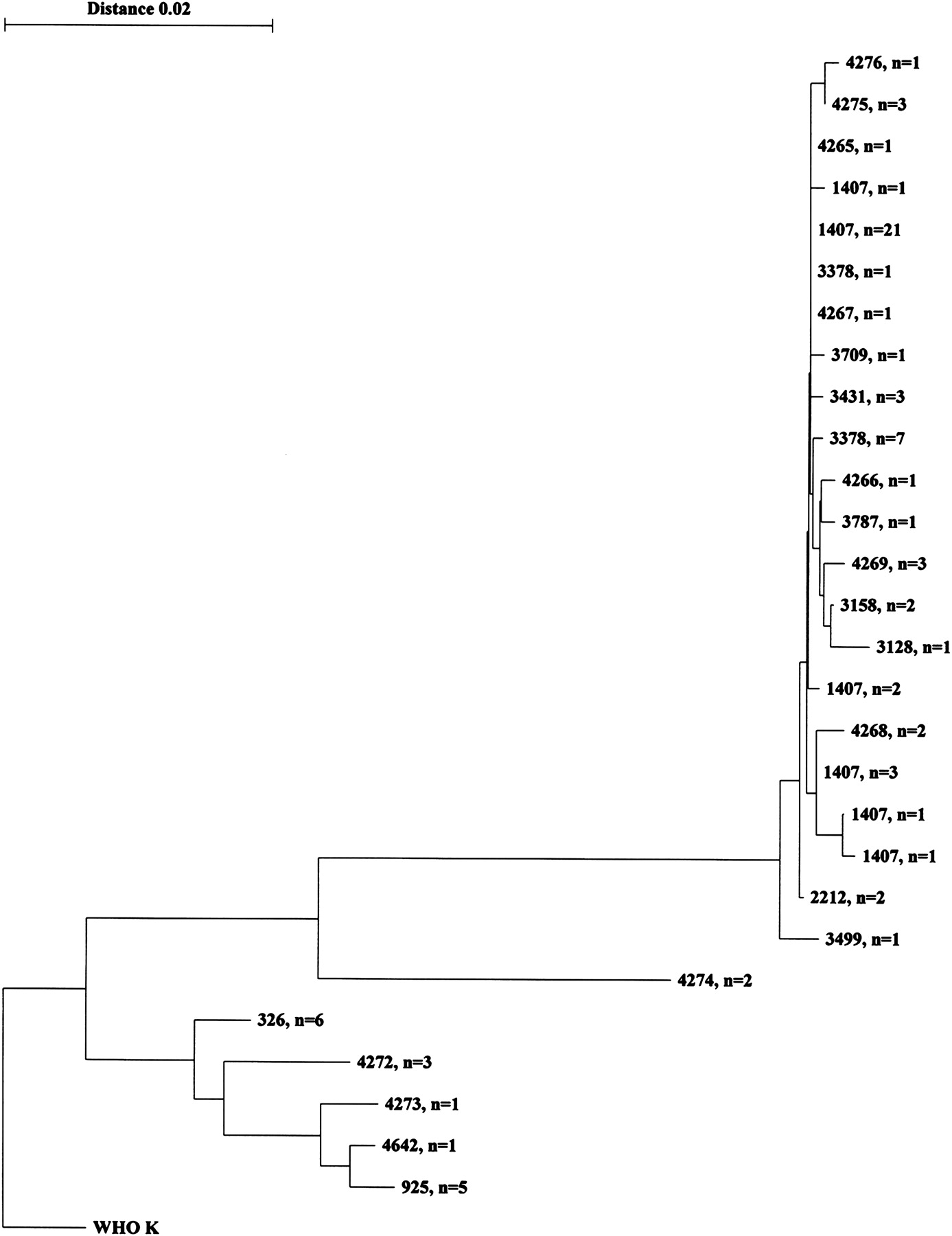
Among the isolates containing a penA mosaic allele (n=78), 22 different NG-MAST sequence types were identified, 11 of which had not been previously described (table 2). However, phylogenetic analysis of the full-length porB gene sequences (25 different sequences) showed that 60 (77%; 90% (60/67) of all found after 2003) of these penA mosaic allele isolates belonged to a cluster comprising all ST1407 (n=29) and very closely related genotypes (n=31), that is differing by a maximum of 14 nucleotides in the full-length porB gene (figure 2). The isolates comprising this cluster were from patients infected in Sweden, many other European Union (EU) and Eastern European countries, the USA, South-East Asia (Thailand), and the WHO WPR (Japan, the Philippines, China, Korea and Australia). Among the isolates with an alteration of A501 in PBP2 (n=37), a total of 16 different sequence types were observed, four of which had not been previously described. These isolates were phylogenetically more heterogeneous (data not shown); however, nine isolates belonged to the identical sequence type (ST1103) (table 2).
{kind=link}
{kind=link}
Phylogenetic tree showing the evolutionary relationships of full-length porB gene sequences of Neisseria gonorrhoeae penA mosaic isolates (n=78) cultured in Sweden in 2002–2009. The 2008 WHO K reference strain,22 comprising a penA mosaic allele X and cultured in Japan in 2001, was used to root the tree. The N gonorrhoeae multiantigen sequence typing (NG-MAST) sequence type (ST) and number of isolates are indicated.
Discussion
In the present study, it has been clearly shown that susceptibility to ESCs (both oral and injectable), the last remaining options for the treatment of gonorrhoea, is rapidly decreasing and, according to the tentative EUCAST breakpoints (http://www.eucast.org), in vitro resistance to both cefixime and ceftriaxone has already been identified in Sweden. Furthermore, it was clearly demonstrated that the decreased susceptibility and resistance to ESCs such as cefixime and ceftriaxone is associated with both penA mosaic alleles and alteration of A501 in PBP2, in synergy with the mtrR and penB resistance determinants, which has been previously reported.1 3 15 However, the effects of the different resistance determinants on the fold-increase in the MICs differ for cefixime and ceftriaxone.15 Interestingly, no clinical N gonorrhoeae isolate with a penA mosaic allele that also contains mutations causing an alteration of A501 in PBP2 has ever been reported. The alteration of A501 in PBP2 still seems to be a gonococcal specific alteration, perhaps due to ESC selection pressure rather than transformation, which may reflect the lower extent of clonal spread observed in the present study. It cannot be excluded that an isolate with a penA mosaic allele that develops mutations resulting in an alteration of A501 has lower biological fitness. However, this is probably not the case and instead it is only a matter of time before these types of strains emerge which may even be resistant to both cefixime and ceftriaxone.
The selection of isolates with MIC values ≥0.032 for cefixime and/or ceftriaxone in the present study made it possible to detect different combinations of the resistance determinants mentioned above. Accordingly, in order to detect isolates containing the initial ESC resistance determinants, that is which cannot be considered as fully susceptible to ESCs, the breakpoints stated by the Clinical and Laboratory Standards Institute (CLSI; http://www.clsi.org) and EUCAST (http://www.eucast.org) are too high. Nevertheless, detection of the initial resistance determinants (penA mosaic alleles or alteration of A501 in PBP2, mtrR and penB alterations) is currently only for surveillance purposes to monitor the emergence and spread of isolates with decreased ESC susceptibility, and not to identify isolates with clinical resistance causing treatment failure. However, this type of surveillance (using lower MIC breakpoints), if possible supplemented by genetic screening for the detection of penA mosaic alleles as well as alterations of A501 in PBP2, in addition to the mtrR and penB determinants, and monitoring of longitudinal trends in ESC MICs over time, would be exceedingly valuable, particularly regarding the emergence and spread of decreased susceptibility and resistance to ESCs, especially ceftriaxone. Alterations in additional genes have been previously suggested to contribute to the decreased susceptibility and resistance to ESCs, such as mutations in pilQ (previously known as penC)27 and mutations in ponA encoding PBP1.3 However, as recent studies have shown that, in contrast to the penicillins, pilQ and ponA alterations do not significantly affect susceptibility to ESCs in N gonorrhoeae15 (DM Whiley, S Jacobsson, JW Tapsall, et al, submitted), these two genes were not examined in the present study. Importantly, in many cases it remains difficult to accurately correlate the known resistance determinants (alterations in penA, mtrR and penB) to the ESC MICs of the isolates.1 3 5 15 Partly this is due to the fact that there are different types of penA mosaic and PBP2 A501 altered alleles, which continue to evolve, and their effects on the ESC MICs of the corresponding gonococcal isolates vary greatly; for example, some A501 altered alleles do not significantly increase the ESC MICs. In addition, the presence or absence of the mtrR and penB resistance determinants further affects the MICs of the ESCs. However, it is also clear that at least one unknown resistance determinant exists and accordingly the mechanisms and their interactions underlying the development of ESC decreased susceptibility and resistance are not all known.1 3 15 Accordingly, enhanced knowledge and better correlates of the genetic resistance determinants, in vitro ESC MICs of the corresponding isolates and treatment outcome, and improved understanding of the spread of isolates with decreased susceptibility and resistance to ESC are essential.
Finally, the present study revealed, using NG-MAST and full-length porB gene sequencing, that several different gonococcal strains with penA mosaic alleles or alterations of A501 in PBP2 are circulating in Sweden and other countries2–4 6 28 29 (also see http://www.ng-mast.net). However, specific gonococcal strains such as ST1407, and its evolving genetically very similar subtypes, containing a penA mosaic allele mostly identical to the penA mosaic allele X associated with treatment failure using oral ESCs in, for example Japan,10 are now increasingly spreading in the WHO WPR, South-East Asia (Thailand), and many EU as well as Eastern European countries and the USA2 4 28 29 (see also http://www.ng-mast.net). Accordingly, a more or less global spread, after initial emergence in the WHO WPR, of some gonococcal penA mosaic allele strains with decreased susceptibility and resistance to ESCs can already be seen.
In conclusion, the number of N gonorrhoeae isolates with decreased susceptibility and resistance to cefixime and ceftriaxone has substantially increased in Sweden over the years. Several different gonococcal strains containing a penA mosaic allele or alterations of A501 in PBP2 with decreased susceptibility to ESCs are circulating in Sweden and other countries. However, specific gonococcal strains such as ST1407, and its evolving genetically very similar subtypes, account for the majority of these isolates. As the scale of the spread is unclear and the amount of treatment failures is unknown, it is essential to more effectively monitor the situation and consider it in a global context.
Key messages
Antimicrobial resistance in gonococci is a major public health problem worldwide, and gonorrhoea may become untreatable in certain circumstances.
Gonococcal susceptibility to extended-spectrum cephalosporins (ESCs), the last remaining treatment options in many settings globally, is rapidly decreasing in Sweden as observed worldwide.
penA mosaic alleles and A501 alterations, together with mtrR and penB, are important for decreased susceptibility/resistance to ESCs; however, unknown resistance determinant(s) also exist.
At least one gonococcal penA mosaic strain (ST1407), including its evolving genetically related subtypes, with decreased susceptibility/resistance to ESCs seems to be circulating worldwide.
References
Footnotes
Funding This study was supported by grants from the Örebro County Council Research Committee and the Foundation for Medical Research at Örebro University Hospital, Sweden.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.